Download to read offline
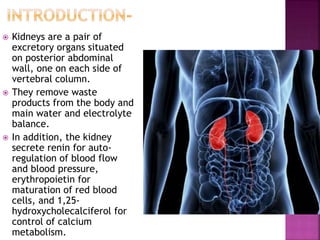
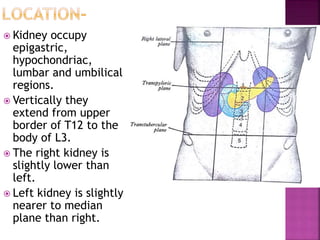
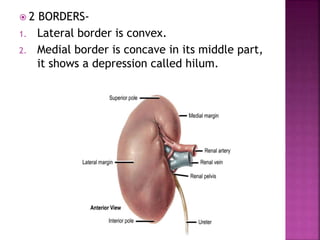
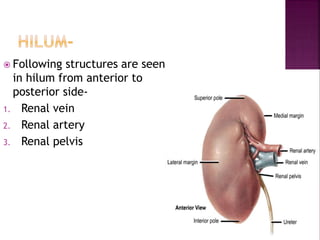
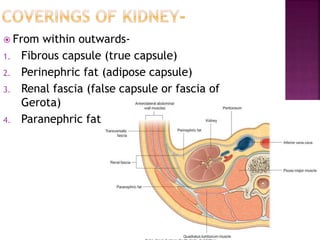
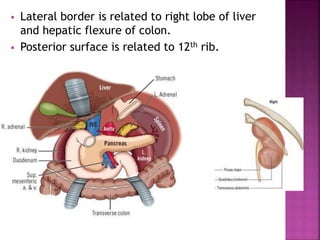
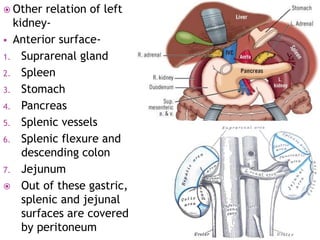
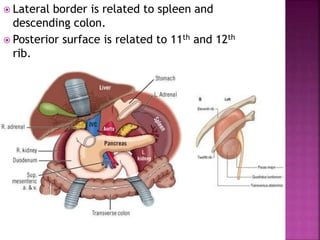
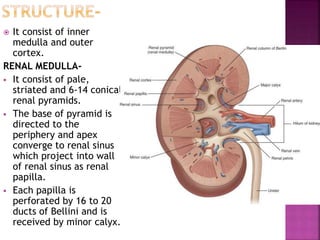
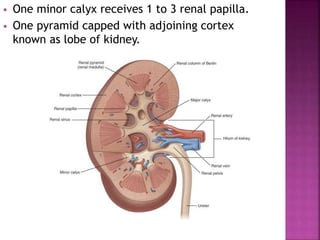
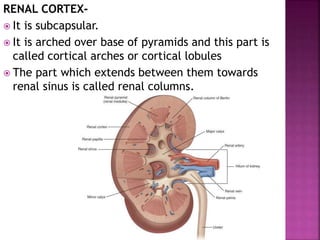
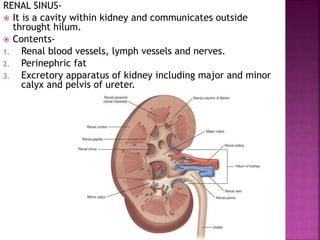
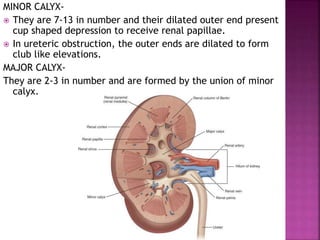
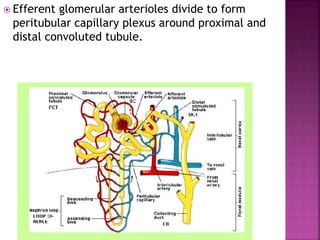
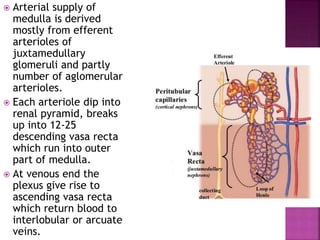
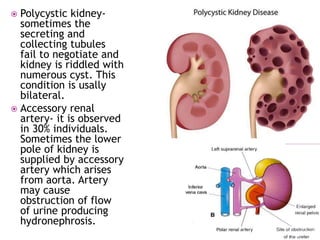



The kidneys are a pair of excretory organs located retroperitoneally on either side of the vertebral column. They remove waste and regulate water and electrolyte balance. Each kidney contains an inner medulla and outer cortex. The kidneys receive blood supply from the renal arteries and drain into the renal veins. They are important for regulating blood pressure and red blood cell production. Kidney diseases can cause hypertension, renal failure and require dialysis in severe cases.
















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















