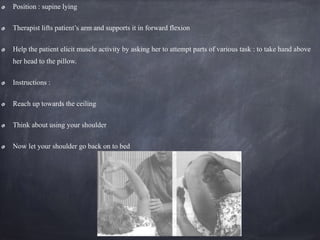
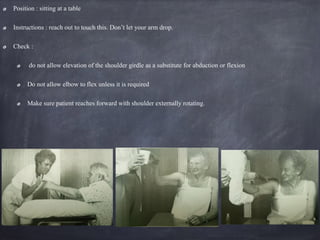
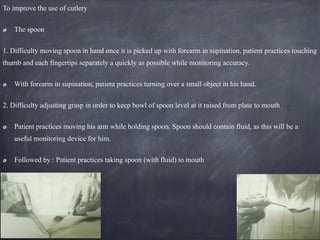
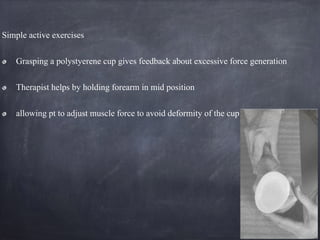
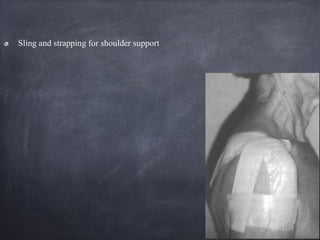
The document outlines a Motor Relearning Program (MRP) developed by physiotherapists Janet Carr and Roberta Shepherd, focusing on the task-oriented relearning of daily activities for stroke patients. Key principles include using a structured rehabilitation plan that emphasizes practice in varied environments, early intervention, and incorporating sensory feedback to improve motor control. Additionally, it discusses mechanisms of recovery, motivational factors in rehabilitation, and specific strategies for training upper limb function post-stroke.