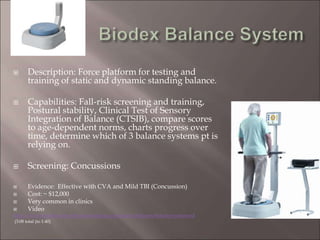
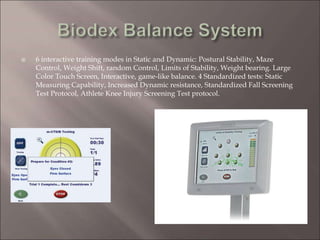
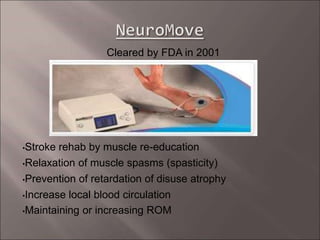
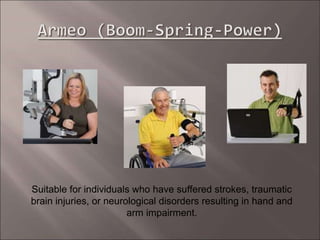
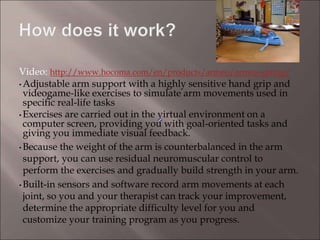
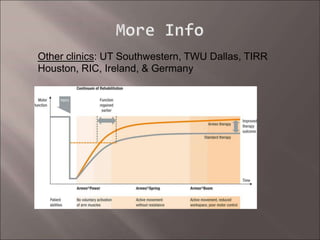
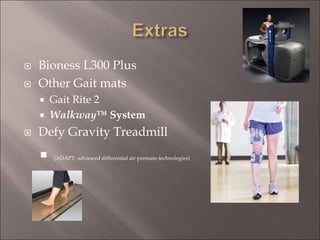
The document introduces recent advances in rehabilitation technology and provides an overview of 11 devices. It discusses how these technologies can provide real-time feedback, objective measures of progress, and engaging rehabilitation. The technologies discussed include the Balancemaster and Biodex Balance System for balance training, Neuromove and Lokomat for gait rehabilitation, and Armeo for arm rehabilitation. Evidence is presented showing that these technologies have been effective for conditions like stroke and concussions when used as part of a comprehensive rehabilitation program.