Download as PDF, PPTX

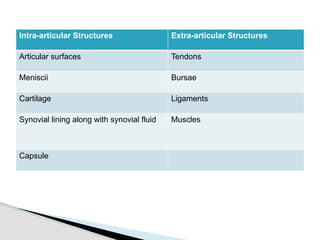



























This document provides an overview of joint structure and function. It defines a joint and lists the intra-articular and extra-articular structures. It describes the basic principles of joint design and complexity matching function. It explains Wolff's law relating bone structure to function. It details the cellular and extracellular components of connective tissue, including collagen and elastin fibers. Finally, it discusses joint classification, motions, and the response of connective tissues to loads.