Download as PDF, PPTX
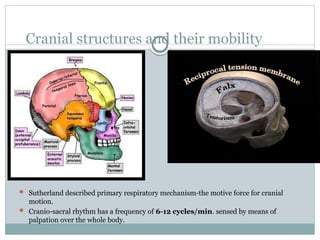
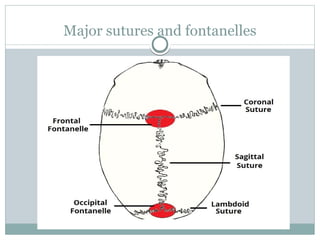
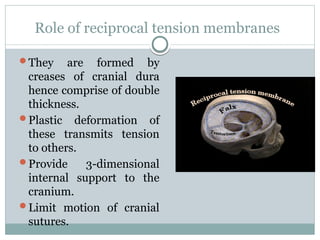
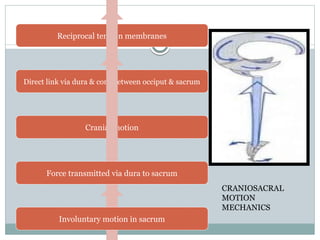
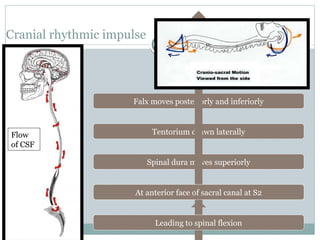
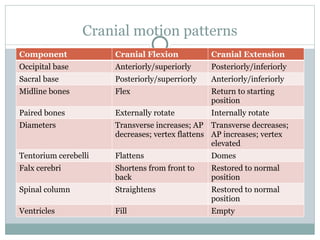
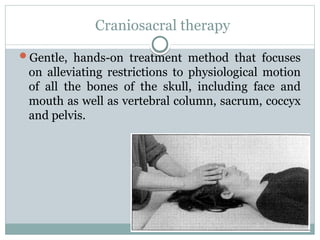
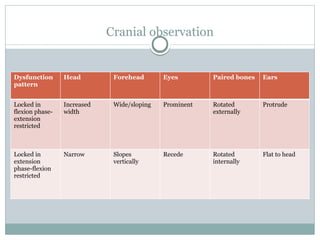
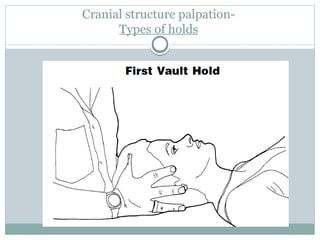
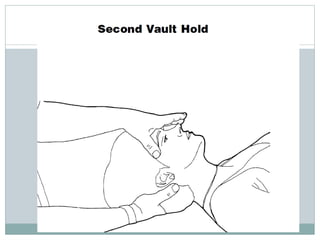
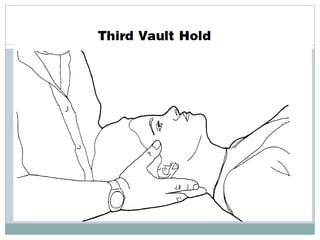


This document provides an overview of craniosacral therapy, including its history, principles, techniques, and applications. It describes how craniosacral therapy involves gentle manual treatment of the cranial bones and spinal column to relieve restrictions and balance the craniosacral rhythm. Key aspects covered include the cranial motion patterns, assessment methods involving palpation of cranial structures, different treatment techniques, indications for its use, and contraindications.























































































