This document discusses weight management in pediatrics. It notes that over 1/3 of US adults and 1/3 of youth are overweight or obese. Obesity is defined as a BMI at or above the 95th percentile, while overweight is between the 85th to 95th percentile. Obesity can lead to health conditions like heart disease and diabetes. Obesity prevalence varies by race, age, sex, education level and other factors. Extra weight can cause sleep issues in children like sleep apnea. Genetics and behaviors are the main causes of excess weight in youth as in adults. The document evaluates a patient's case and provides a treatment plan focusing on nutrition education and physical activity goals.
Soraya Ghebleh - Strategies to Reduce Childhood ObesitySoraya Ghebleh
This is a presentation from Soraya Ghebleh that looks at the problem of childhood obesity in America and offers potential policy and strategy solutions.
Soraya Ghebleh - Strategies to Reduce Childhood ObesitySoraya Ghebleh
This is a presentation from Soraya Ghebleh that looks at the problem of childhood obesity in America and offers potential policy and strategy solutions.
Childhood Obesity Prevention: What's the Evidence?Health Evidence™
Presented as part of a Canadian Institutes of Health funded Knowledge Translation Supplement grant (KTB-112487) (1 of 8 webinars). Recorded May 23, 2012.
Research project presentation By David Bandi Julius Leyi 2021DavidBandiJulius
Brief summary of my reasearch draft work. The research was conducted by a student who is currenty finishing his degree. it is just the sample of unfinished research work i.e it is under corrections. https://www.youtube.com/channel/UC0wEQw2nvXuVBDiGhH_8AtQ?sub_confirmation=1
Childhood Obesity Prevention: What's the Evidence?Health Evidence™
Presented as part of a Canadian Institutes of Health funded Knowledge Translation Supplement grant (KTB-112487) (1 of 8 webinars). Recorded May 23, 2012.
Research project presentation By David Bandi Julius Leyi 2021DavidBandiJulius
Brief summary of my reasearch draft work. The research was conducted by a student who is currenty finishing his degree. it is just the sample of unfinished research work i.e it is under corrections. https://www.youtube.com/channel/UC0wEQw2nvXuVBDiGhH_8AtQ?sub_confirmation=1
Bell's palsy is a form of temporary facial paralysis resulting from damage or trauma to the facial nerves. The facial nerve-also called the 7th cranial nerve-travels through a narrow, bony canal (called the Fallopian canal) in the skull, beneath the ear, to the muscles on each side of the face. For most of its journey, the nerve is encased in this bony shell.
Each facial nerve directs the muscles on one side of the face, including those that control eye blinking and closing, and facial expressions such as smiling and frowning. Additionally, the facial nerves carries nerve impulses to the lacrimal or tear glands, the saliva glands, and the muscles of a small bone in the middle of the ear called the stapes. The facial nerve also transmits taste sensations from the tongue.
When Bell's palsy occurs, the function of the facial nerve is disrupted; causing an interruption in the messages the brain sends to the facial muscles. This interruption results in facial weakness or paralysis.
Bell's palsy is named for Sir Charles Bell, a 19th century Scottish surgeon who was the first to describe the condition. The disorder, which is not related to stroke, is the most common cause of facial paralysis. Generally, Bell's palsy affects only one of the paired facial nerves and one side of the face, however, in rare cases, it can affect both sides.
Clinical Research Challenges and Best Practices in Pediatric Research in Canada - Dr. Al Wahab - 2015
Dr. Zeina AlWahab, M.D.
Prof. Peivand Pirouzi, Ph.D., M.B.A.
Childhhood Obesity ppt Presentation Slide 2024.pptMotahar Alam
Childhood obesity is a significant health concern characterized by excessive body fat accumulation in children and adolescents. It results from a complex interplay of genetic, behavioral, environmental, and socioeconomic factors. Obesity in childhood is typically determined by measuring body mass index (BMI), which compares a child's weight to their height.
The prevalence of childhood obesity has been steadily rising globally over the past few decades, becoming one of the most pressing public health challenges of the 21st century. This trend is alarming because obesity during childhood is associated with various immediate and long-term health consequences.
Physically, obese children are at a higher risk of developing numerous health problems such as type 2 diabetes, high blood pressure, asthma, sleep apnea, joint problems, and fatty liver disease. Psychologically, they may experience low self-esteem, depression, and social stigma, which can significantly impact their overall well-being and quality of life.
The causes of childhood obesity are multifaceted. Sedentary lifestyles characterized by excessive screen time, lack of physical activity, and poor dietary habits high in calorie-dense, nutrient-poor foods contribute significantly to its prevalence. Additionally, genetic predisposition, parental influences, socioeconomic status, and environmental factors such as access to healthy foods and safe outdoor spaces play crucial roles.
Preventing and addressing childhood obesity require a comprehensive, multi-sectoral approach involving families, schools, healthcare providers, policymakers, and the food and beverage industry. Strategies may include promoting healthy eating habits, increasing physical activity opportunities, implementing policies to improve food environments, providing education and support to families, and fostering community-wide initiatives.
Aene project a medium city public students obesity studyCIRINEU COSTA
Identifying undernutrition and obesity on students and propose public policies of health are urgent issues. This paper presents a study with weight and stature from students collected by physical education teachers (PEF) in schools of a city near São Paulo. The PEF collected the data and they were inserted in a program especially developed for each school Department (AENE Project). The datas were analyzed by software and evaluation done based on a World Health Organization (WHO_2007) table, that develops health programs worldwide. The results evaluations were used to raise the students and family, teachers and responsibles for treatment search (when required).
http://www.unileverhealth.co.za/about | There are 195 million children in the world who have not developed adequately and are too short for their age. There are also 42 million children below the age of five who are obese. What all these children have in common is that they have not received the right nutrition growing up. That is why Unilever Health has made child nutrition one of its main focus points. Unilever prides itself on producing products that are conducive to a child’s development and educating people on the nutrition needs of children.
1. Jennifer Derasmo
Nutrition Sciences Student
Weight Management in Pediatrics
• More than one-third (34.9% or 78.6 million) of U.S.
adults are obese. (2) One-third of youths are
overweight or obese. (1)
• The term “obese” describes children and
adolescents who have a body mass index (BMI) at
or above the 95th percentile for their gender and
age, while “overweight” describes those with a
BMI at or above the 85th but below the 95th
percentile. (1)
• Obesity-related conditions include heart disease,
stroke, type 2 diabetes and certain types of cancer,
some of the leading causes of preventable death.
(2)
Pathophysiology
Obesity prevalence differs among racial/ethnic
groups and also varies by age, sex, and adult head of
household’s and education level (3)
According to the National Sleep Foundation (NSF),
extra pounds on children can put them at risk for
Obstructive Sleep Apnea (OSA) which affects mood,
difficulty in concentrating at school, headaches and
changes in performance (4)
The main causes of excess weight in youth are
similar to those in adults, including individual causes
such as behavior and genetics (5)
• Adipex-anorexiant, CNS stimulant, may cause dry mouth
and an unpleasant taste
• Alli- fat malabsorption,peripherally acting antiobesity
agent, may cause diarrhea, loss of appetite, nausea, sore
throat, vomiting, tooth problems, swelling of lips,
tongue, throat, and abdominal pain.
• Belviq- Anorexiants, CNS stimulants, may cause
increased and painful urination, sore throat, dry mouth,
increased hunger, rapid weight gain, unusual weight
1. NCCOR Childhood Obesity in the United States. (n.d.).
Retrieved February 10, 2016, from http://www.nccor.org/
2. Adult Obesity Facts. (2015). Retrieved March 09, 2016, from
http://www.cdc.gov/obesity/data/adult.html
3. Childhood Obesity Facts. (2015). Retrieved March 09, 2016,
from http://www.cdc.gov/obesity/data/childhood.html
4. Children and Sleep. (n.d.). Retrieved March 07, 2016, from
https://sleepfoundation.org/sleep-topics/children-and-sleep
5. Childhood Obesity Causes & Consequences. (2015). Retrieved
March 02, 2016, from
http://www.cdc.gov/obesity/childhood/causes.html
Background
Drugs & Supplements
Financial Impact
• The annual nationwide productive costs of obesity
obesity-related absenteeism range between $3.38
billion
• Childhood obesity comes with an estimated price tag
of $19,000 per child (2)
• Childhood obesity alone is responsible for $14 billion
in direct medical costs (2)
References
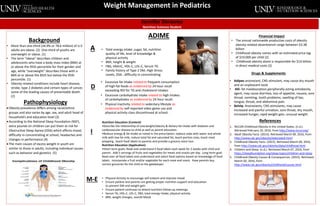
ADIME
• Total energy intake ,sugar, fat, nutrition
quality of life, level of knowledge &
physical activity
• BMI, height & weight
• FBG, HbA1C, HDL-C, LDL-C, Serum TG
• Family history of Type 2 DM, High Stress
Levels, OSA , difficulty in concentrating
D
I
M-E
• Excessive fat intake related to frequent consumption
of high-fat foods as evidenced by 24 hour recall
exceeding RDI for TG and cholesterol intakes.
• Excessive carbohydrate intake related to high intakes
of carbohydrates as evidenced by 24 hour recall.
• Physical inactivity related to sedentary lifestyle as
evidenced by self-reported video game use and
physical activity class discontinued at school.
Nutrition Education (Content)
•Describe the relationship of overweight/obesity & dietary fat intake with diabetes and
cardiovascular disease to child as well as parent education
•Reduce energy & fat intake as noted in the prescription, replace soda with water and whole
milk with low fat milk, reduce total fat and saturated fat, teach portion sizes, teach meal
prepping , teach food labels to parents and provide a grocery store tour
Nutrition Education (Application)
•Short term goals: Read and understand 4 food labels each week for 2 weeks with child and
parent. Add 5 servings of fruits and vegetables for meals and snacks per day. Long-term goal:
Read over all food labels and understand and select food options based on knowledge of food
labels. Incorporate a fruit and/or vegetable for each meal and snack. Have parents buy
correct groceries for the child as the gatekeeper.
• Physical Activity to encourage self-esteem and improve mood
• Ensure patient and parents are getting proper nutrition support and education
to prevent DM and weight gain
• Ensure patient continues to attend nutrition follow-up meetings
• Serum TG, HDL-C, LDL-C, FBG, total energy intake, physical activity
• BMI, weight changes, overall Mood
A