Downloaded 992 times


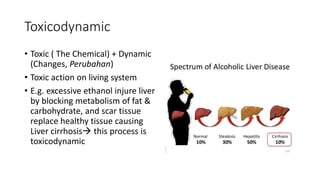
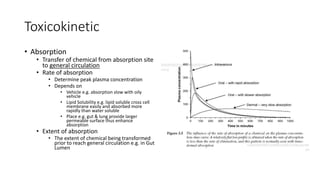



Toxicology is the study of how poisons affect living organisms. Some key points: - Toxicology has a long history dating back to the 15th century physician Paracelsus who said "the dose makes the poison." - Toxicants can enter the body through various routes like skin contact, inhalation, or ingestion and cause local or systemic effects. - Toxicants are classified into categories like heavy metals, solvents, radiation, pesticides, and plant/animal toxins. Each can have acute and chronic health effects depending on dose and route of exposure. - Toxicokinetics refers to how the body absorbs, distributes, and eliminates toxins while


















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



