Downloaded 526 times


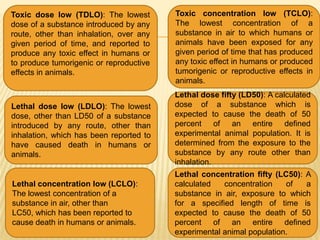

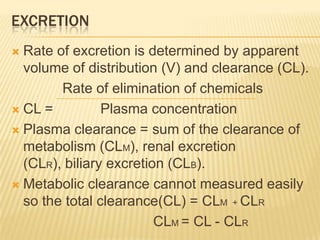



The document provides an overview of toxicology. It defines toxicology as the study of adverse effects of chemicals and physical agents on living organisms. Key points include: - Toxicology studies mechanisms of toxicity, risk factors, and safety measures for toxic substances. It aims to qualitatively identify hazards and quantitatively determine exposure conditions. - Important figures in the history of toxicology include Paracelsus, who established the concept that the dose makes the poison, and Mathieu Orfila, considered the modern father of toxicology. - Toxicity is measured using various endpoints like mortality, teratogenicity, carcinogenicity, and mutagenicity. Metrics like LD50, TDLO,
















































































