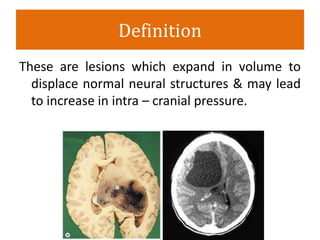
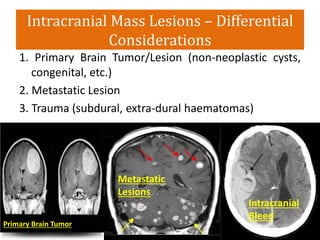
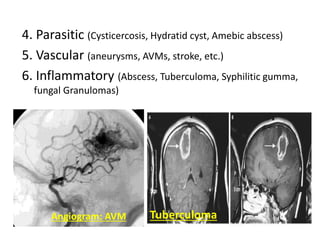
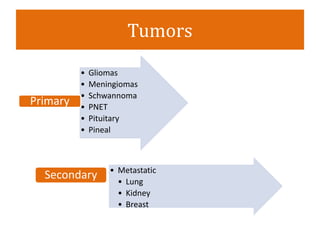
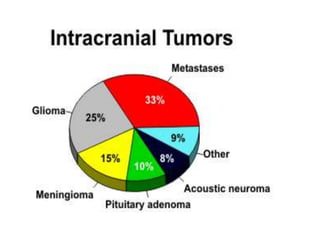
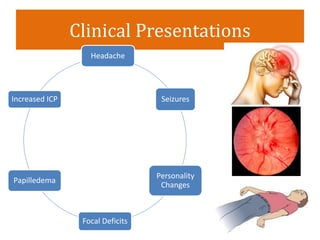
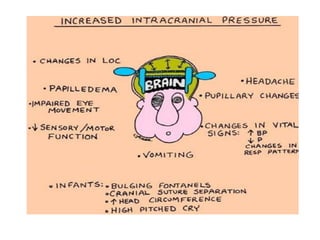
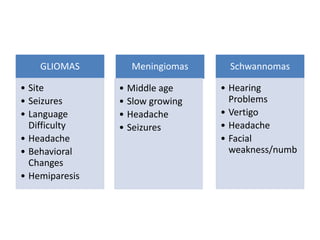
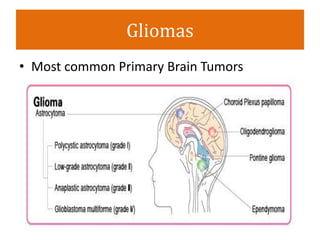
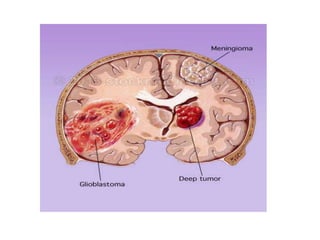
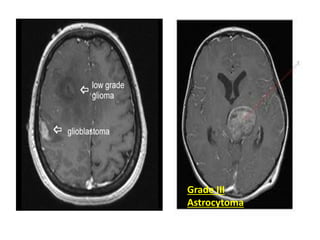
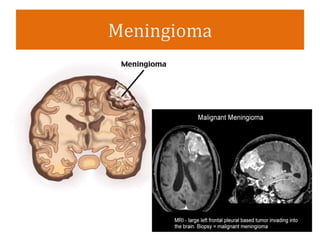
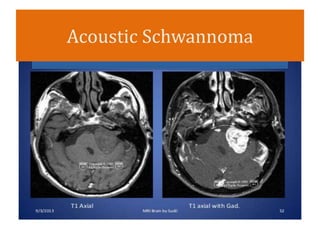
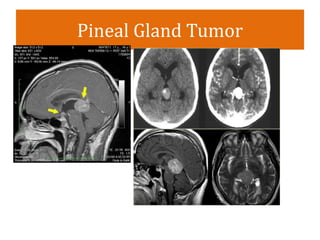
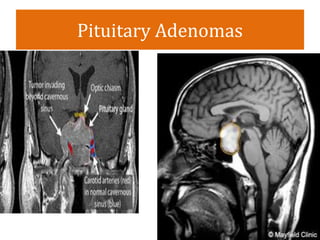
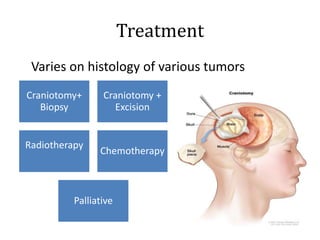
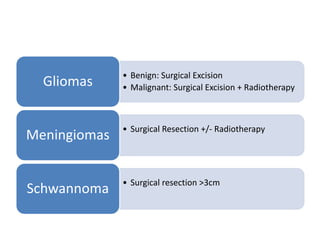
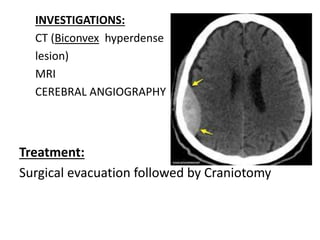
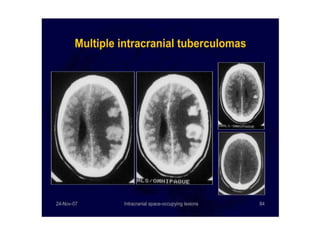
This document discusses intracranial space occupying lesions, including their definition, types, clinical presentations, diagnosis, and treatment. It defines these lesions as those that expand in volume to displace normal neural structures and may increase intracranial pressure. It then describes the main types of lesions such as primary and metastatic brain tumors, traumatic injuries like hematomas, and infectious or inflammatory causes. The clinical presentations, diagnosis using imaging and other tests, and treatment approaches are outlined for each of the major lesion types. Surgical resection and other procedures are discussed as primary treatment methods depending on the specific lesion.