Downloaded 224 times
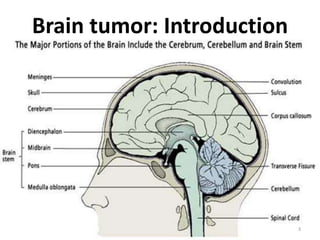















This document provides information about brain tumors. It defines a brain tumor as a localized intracranial lesion that occupies space within the skull and causes increased intracranial pressure. It discusses the types of brain tumors, which include gliomas, meningiomas, and pituitary adenomas. The signs and symptoms of brain tumors can include headaches, seizures, nausea and vomiting, and changes in vision, speech, or hearing. Diagnosis involves medical imaging like CT scans and MRIs. Treatment may involve surgery to remove the tumor, radiation therapy, and chemotherapy. Nursing management focuses on assessing neurological status, preventing complications like increased intracranial pressure, and providing pre- and post-operative care.






























































