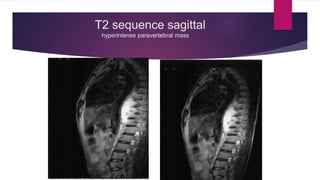
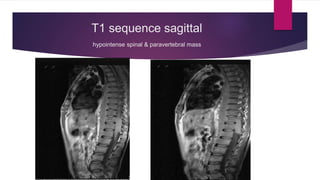
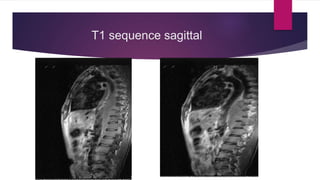
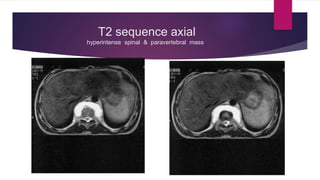
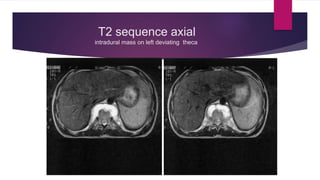
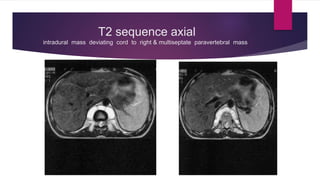
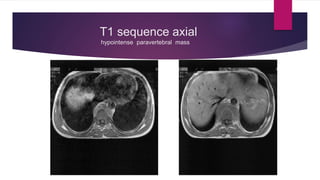
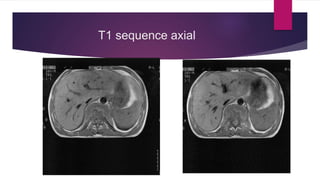
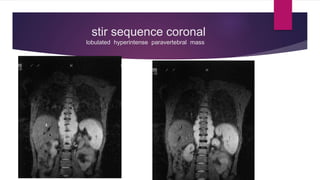
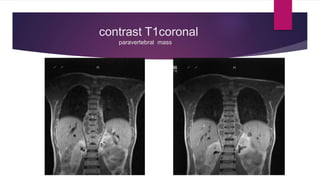
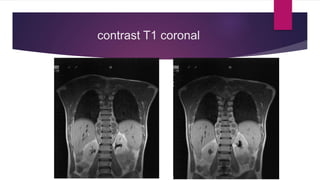
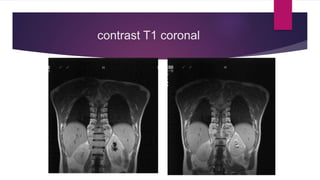
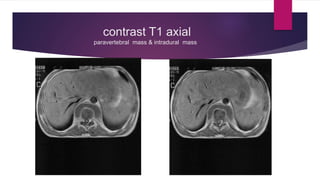
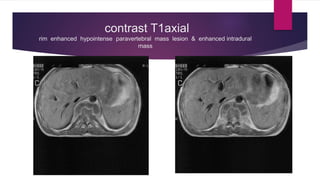
An 18-year-old boy presented with 6 months of lower back pain and lower extremity weakness on the left side. MRI revealed two masses - an intradural extramedullary mass between D10-D12 deviating the spinal cord to the right, and a long paravertebral mass extending from T7-L1. The intradural mass enhanced with contrast and was considered to be an intradural extramedullary lesion such as a neurofibroma. The patient was referred for surgical management and biopsy to determine the exact diagnosis.