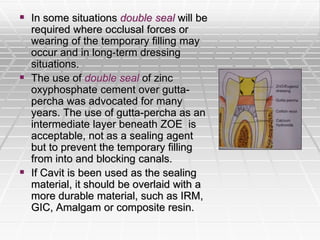
This document discusses intracanal medications used during root canal treatment. It begins by outlining the rationale for using intracanal medications, which is to help kill remaining bacteria and prevent reinfection between appointments. The document then describes various classes of antibacterial agents that have been used, including antibiotics, alcohols, phenolic compounds, heavy metals, cationic detergents, halogens, and steroids. It focuses on the functions, modes of action, benefits and limitations of common medications like sodium hypochlorite, camphorated phenol, and calcium hydroxide.