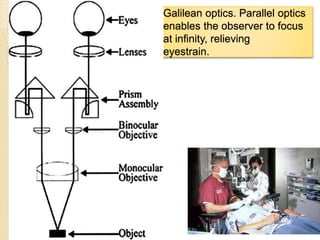
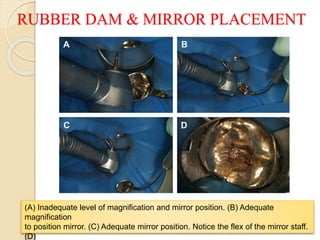
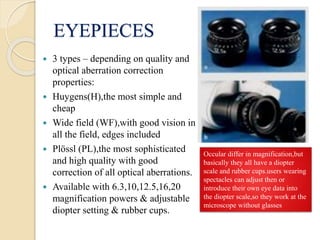
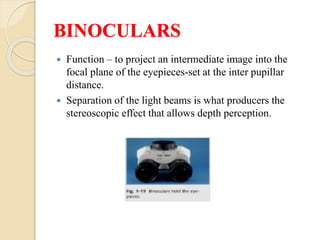
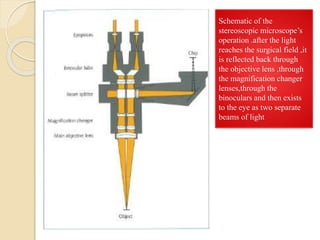
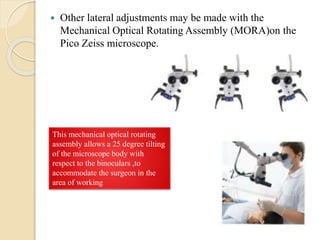
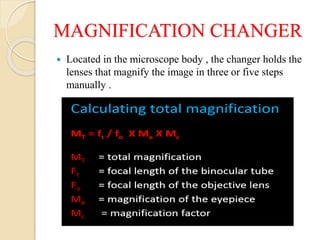
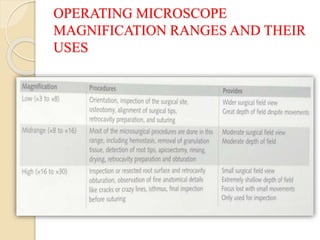
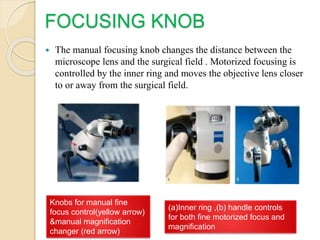
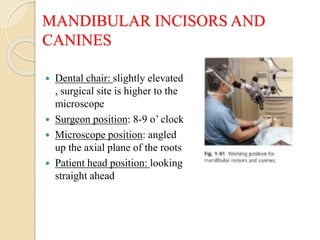
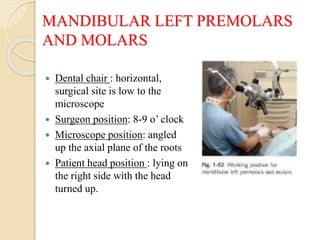
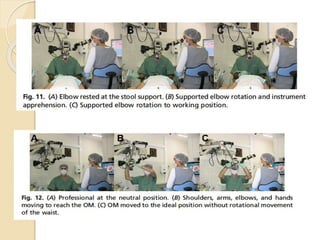
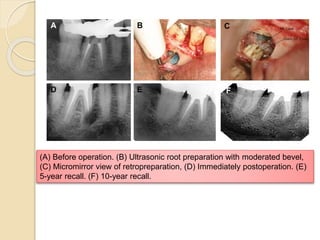
The document discusses the use of dental operating microscopes (DOM) in dentistry. It describes the key parts of a DOM including eyepieces, binoculars, magnification changer, and objective lens. Advantages of DOM include increased diagnostic ability, reduced trauma, and marketing benefits. Ergonomic working positions and appropriate use of magnification ranges for different procedures are discussed. The conclusion emphasizes the importance of understanding ergonomics and acquiring skills when adopting the use of an DOM.




































![Principles of periodontal instrumentation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/principlesofperiodontalinstrumentationautosaved-210220074109-thumbnail.jpg?width=640&height=640&fit=bounds)



































