Downloaded 155 times


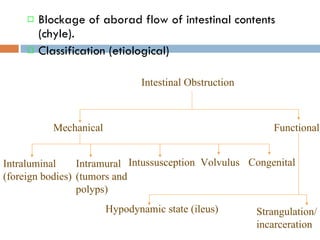






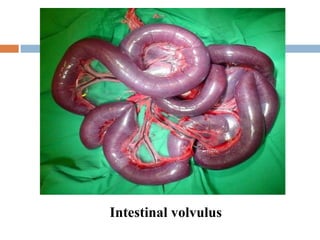
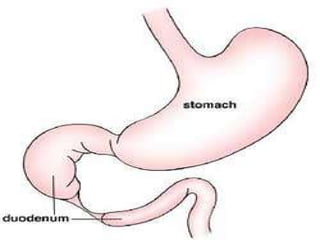
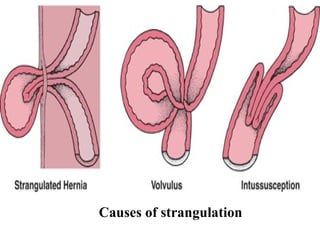



The document summarizes intestinal obstruction in animals, including its classification, signs, diagnosis, and treatment. Intestinal obstruction can be mechanical, functional, intraluminal, intramural, or congenital. Signs depend on the location and severity of the obstruction. Diagnosis involves history, clinical examination, imaging like radiography and ultrasound, and laboratory tests. Treatment involves fluid therapy, surgery to remove obstructions, and managing complications like strangulation and peritonitis.
















































































