AN OVERVIEW OFINTELLECTUAL
DISABILITY
Moderator: Dr. S. Ghosh
Associate professor
Presentor: Dr. Pinky Poddar
Post graduate trainee
Department of psychiatry, AMCH
2.
PLAN OF PRESENTATION
Introduction
History
Definition of Intellectual Disability
Levels of Intellectual Disability
Epidemiology
Etiology
Developmental Considerations
Genetic Intellectual Disability Syndromes and Behavioral Phenotypes
Psychiatric illness and intellectual disability
Management
Role of psychiatrists
Services and support
Legal Issues
Conclusion
Bibliography
3.
INTRODUCTION
Intellectual disabilityis a disability that causes significant
limitations both in intellectual functioning and in adaptive
behaviour as expressed in conceptual,social and practical
adaptive skills.
Prevalence is 1-3% of population.
More prevalent in lower socioeconomic and in minority
groups.
A number of people with intellectual disability are mildly
affected, making the disability difficult to recognize
without visual cues.
4.
Intellectual disabilityis diagnosed through the use of
standardized tests of intelligence and adaptive
behavior.
Individuals with intellectual disabilities who are
provided appropriate personalized supports over a
sustained period generally have improved life
outcomes.
In fact, many adults with intellectual disabilities can live
independent, productive lives in the community with
support from family and friends.
5.
HISTORY
The understandingof persons with intellectual
disability has moved like a pendulum between
extremes.
At one end, persons with intellectual disability have
been exalted, and considered “Les enfants du Bon Dieu”
(“children of the Good God”).
And at the other end of the pendulum swing, such
persons have also been vilified with words like
“stupid, vulgar, and insensitive.”
6.
The earliestreference to intellectual disability dates to
the Egyptian Papyrus of Thebes in 1552 B.C.(Harris
2006)
The oldest psychological view of intellectual disability
is in the writings of Hippocrates in the late 5th
century
B.C. who believed that it was caused by an imbalance
in the four humors in the brain.
In the 17th
century, Thomas Willis provided the first
description of intellectual disabilities as a disease . He
believed it was caused by structural abnormality in
brain.
7.
Esquirol (1838),is credited as the first medical writer to
define the disorder and he was careful to distinguish
intellectual disability from mental illness or disease.
He focused on congenital onset in noting that:
“Idiocy is not a disease, but a condition in which the
intellectual faculties are never manifested;
or
have never been developed sufficiently to enable the
idiot to acquire such an amount of knowledge as
persons of his own age.
8.
The modernhistory for the field of intellectual
disability begins in the late 18th and early 19th
centuries.
At that time, Jean-Marc Itard attempted a natural
experiment to educate Victor, a “wild-child”
discovered in the forests of Aveyron, France.
His experiment marked the important consideration
that persons with disabilities might be educable.
9.
Early inthe 20th
century, the eugenics movement
became popular throughout the world which led to
forced sterilization and prohibition of marriage in most
of the developed world and was later used by Adolf
Hitler as a rationale for the mass murder of
intellectually challenged individuals during the
Holocaust.
10.
Also playingan important role in intellectual disability research was
the science of psychological testing.
Nearly a century ago, psychologists invented tests of motor,
nonverbal intelligence, achievement, adaptive behavior, and other
skills.
In addition, many studies now examine the presence of psychiatric
disorders in children and adults with intellectual disability, and
families, schools, group homes, and workshops have all received
research attention.
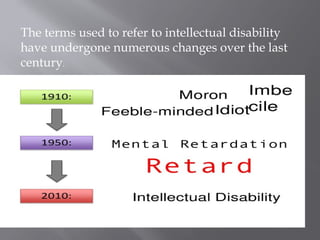
The terms usedto refer to intellectual disability
have undergone numerous changes over the last
century.
14.
DEFINITION (ICD 10AND WHO,1992)
ID or mental retardation is defined :
as a condition of arrested or incomplete development of
the mind,
especially characterized by impairment of skills
manifested during the developmental period,
which contribute to the overall level of intelligence, i.e.,
cognitive, language, motor, and social abilities.
16.
DSM 5(intellectual disability)
INTELLECTUAL
FUNCTION
ADAPTIVEFUNCTION ONSET
Deficits in intellectual
function
reasoning,
problem solving,
planning,
abstract thinking,
judgment,
academic learning,
learning from experience,
Confirmed by
clinical assessment
Intelligence testing.
Deficits in adaptive functioning
failure to meet developmental
and socio-cultural standards for
personal independence and social
responsibility.
limit functioning in one or more
activities of daily life, such as
communication, social
participation,
limit independent living across
multiple environments, such as
home, school, work, and
community.
During the
developmental
period
17.
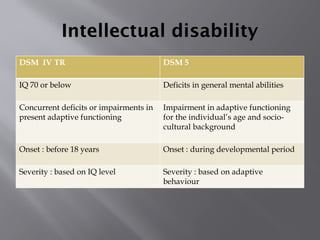
Intellectual disability
DSM IVTR DSM 5
IQ 70 or below Deficits in general mental abilities
Concurrent deficits or impairments in
present adaptive functioning
Impairment in adaptive functioning
for the individual’s age and socio-
cultural background
Onset : before 18 years Onset : during developmental period
Severity : based on IQ level Severity : based on adaptive
behaviour
18.
ADAPTIVE FUNCTIONING
Refersto how effectively individuals cope with
everyday life demands
and
How well they meet standards of personal
independence expected of someone of that age and
socioeconomic and cultural background.
20.
Influenced by anumber of factors
Motivation.
Personality style.
Education.
Social and vocational opportunities.
General medical conditions and mental disorders
that co-exist with Intellectual disability.
21.
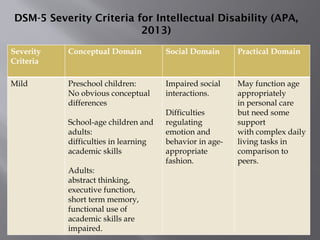
DSM-5 Severity Criteriafor Intellectual Disability (APA,
2013)
Severity
Criteria
Conceptual Domain Social Domain Practical Domain
Mild Preschool children:
No obvious conceptual
differences
School-age children and
adults:
difficulties in learning
academic skills
Adults:
abstract thinking,
executive function,
short term memory,
functional use of
academic skills are
impaired.
Impaired social
interactions.
Difficulties
regulating
emotion and
behavior in age-
appropriate
fashion.
May function age
appropriately
in personal care
but need some
support
with complex daily
living tasks in
comparison to
peers.
22.
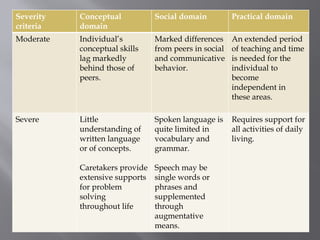
Severity
criteria
Conceptual
domain
Social domain Practicaldomain
Moderate Individual’s
conceptual skills
lag markedly
behind those of
peers.
Marked differences
from peers in social
and communicative
behavior.
An extended period
of teaching and time
is needed for the
individual to
become
independent in
these areas.
Severe Little
understanding of
written language
or of concepts.
Caretakers provide
extensive supports
for problem
solving
throughout life
Spoken language is
quite limited in
vocabulary and
grammar.
Speech may be
single words or
phrases and
supplemented
through
augmentative
means.
Requires support for
all activities of daily
living.
23.
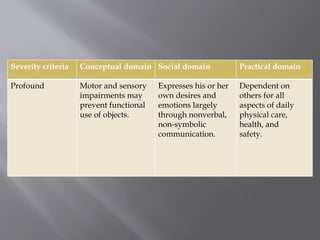
Severity criteria Conceptualdomain Social domain Practical domain
Profound Motor and sensory
impairments may
prevent functional
use of objects.
Expresses his or her
own desires and
emotions largely
through nonverbal,
non-symbolic
communication.
Dependent on
others for all
aspects of daily
physical care,
health, and
safety.
24.
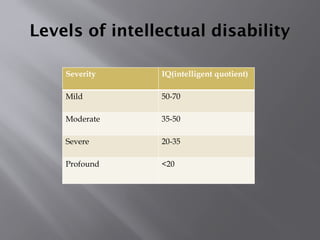
Levels of intellectualdisability
Severity IQ(intelligent quotient)
Mild 50-70
Moderate 35-50
Severe 20-35
Profound <20
26.
Proposed ICD 11criteria for
intellectual developmental disorder
Presence of significant limitations in intellectual
functioning.
Presence of significant limitations in adaptive
behaviour.
Onset during development period.
27.
ICD 11 proposedclassification of IDD
Disorder of intellectual disability, marked
Disorder of intellectual disability,extensive
Disorder of intellectual disability,pervasive
Disorder of intellectual disability,other
28.
Epidemiology
Affects approximately1-4% of the population in
developed countries.
2% of Indian population constitutes persons with
intellectual disability.
According to 2011 census data, there are currently
1,505,624 mentally retarded people in India.
Incidence is 3.1% in rural areas and 0.9% in urban.
1.5 times more common in males.
Children with intellectualdisability traverse the
same sequences in their development as do
children with typical development, but
in certain forms of intellectual disability, there are
strengths and weaknesses not generally found in
typically developing children.
certain slowed development is seen in specific types
of intellectual disability
34.
Typically developingchildren show a specific, possibly
universal, ordering to their development.
For example, in Piagetian cognitive development,
children proceed from
Sensorimotor
preoperational
concrete operational
formal operational thought
35.
Children withintellectual disability also follow a “similar
sequence”
Similar sequences even hold for those children with
genetic or other organic causes for their intellectual
disability.
The only possible exceptions include
some children with uncontrollable seizures (where
accurate testing is difficult),
some children with autism, who may show different
orderings due to their particular disabilities on certain
social tasks.
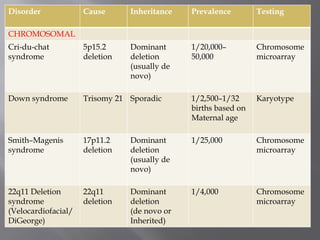
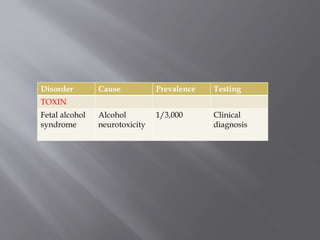
Disorder Cause InheritancePrevalence Testing
CHROMOSOMAL
Cri-du-chat
syndrome
5p15.2
deletion
Dominant
deletion
(usually de
novo)
1/20,000–
50,000
Chromosome
microarray
Down syndrome Trisomy 21 Sporadic 1/2,500–1/32
births based on
Maternal age
Karyotype
Smith–Magenis
syndrome
17p11.2
deletion
Dominant
deletion
(usually de
novo)
1/25,000 Chromosome
microarray
22q11 Deletion
syndrome
(Velocardiofacial/
DiGeorge)
22q11
deletion
Dominant
deletion
(de novo or
Inherited)
1/4,000 Chromosome
microarray
38.
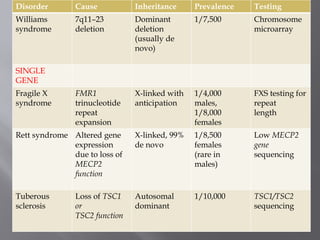
Disorder Cause InheritancePrevalence Testing
Williams
syndrome
7q11–23
deletion
Dominant
deletion
(usually de
novo)
1/7,500 Chromosome
microarray
SINGLE
GENE
Fragile X
syndrome
FMR1
trinucleotide
repeat
expansion
X-linked with
anticipation
1/4,000
males,
1/8,000
females
FXS testing for
repeat
length
Rett syndrome Altered gene
expression
due to loss of
MECP2
function
X-linked, 99%
de novo
1/8,500
females
(rare in
males)
Low MECP2
gene
sequencing
Tuberous
sclerosis
Loss of TSC1
or
TSC2 function
Autosomal
dominant
1/10,000 TSC1/TSC2
sequencing
39.
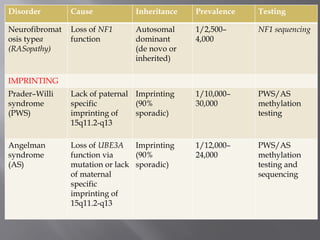
Disorder Cause InheritancePrevalence Testing
Neurofibromat
osis typea
(RASopathy)
Loss of NF1
function
Autosomal
dominant
(de novo or
inherited)
1/2,500–
4,000
NF1 sequencing
IMPRINTING
Prader–Willi
syndrome
(PWS)
Lack of paternal
specific
imprinting of
15q11.2-q13
Imprinting
(90%
sporadic)
1/10,000–
30,000
PWS/AS
methylation
testing
Angelman
syndrome
(AS)
Loss of UBE3A
function via
mutation or lack
of maternal
specific
imprinting of
15q11.2-q13
Imprinting
(90%
sporadic)
1/12,000–
24,000
PWS/AS
methylation
testing and
sequencing
40.
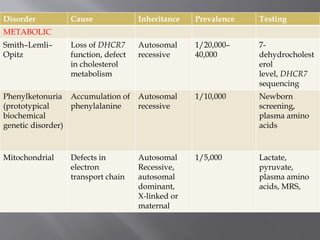
Disorder Cause InheritancePrevalence Testing
METABOLIC
Smith–Lemli–
Opitz
Loss of DHCR7
function, defect
in cholesterol
metabolism
Autosomal
recessive
1/20,000–
40,000
7-
dehydrocholest
erol
level, DHCR7
sequencing
Phenylketonuria
(prototypical
biochemical
genetic disorder)
Accumulation of
phenylalanine
Autosomal
recessive
1/10,000 Newborn
screening,
plasma amino
acids
Mitochondrial Defects in
electron
transport chain
Autosomal
Recessive,
autosomal
dominant,
X-linked or
maternal
1/5,000 Lactate,
pyruvate,
plasma amino
acids, MRS,
41.
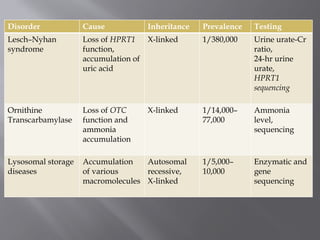
Disorder Cause InheritancePrevalence Testing
Lesch–Nyhan
syndrome
Loss of HPRT1
function,
accumulation of
uric acid
X-linked 1/380,000 Urine urate-Cr
ratio,
24-hr urine
urate,
HPRT1
sequencing
Ornithine
Transcarbamylase
Loss of OTC
function and
ammonia
accumulation
X-linked 1/14,000–
77,000
Ammonia
level,
sequencing
Lysosomal storage
diseases
Accumulation
of various
macromolecules
Autosomal
recessive,
X-linked
1/5,000–
10,000
Enzymatic and
gene
sequencing
Health problems associatedwith
intellectual disability
Compared with normal children, children with ID are
at a higher risk of having other health problems.
The most prevalent health conditions are:
Epilepsy (22%)
Cerebral palsy (20%)
Anxiety disorders (17%)
Oppositional defiant disorder (12%)
Autistic disorder (10%)
(Oeseburg et al,2011)
44.
Epilepsy14-44% higherin more severe ID.
Combination of ID and epilepsy is a strong predictor of
psychiatric and behavioural problems.
Hypothyroidism is common in Down syndrome.
45.
Stomach cancer,and cancer of gall bladder, oesophagus,
testis, thyroid and connective tissue all occur with
greater frequency.
Visual problems 10 times more common.
Cataract and keratoconus also common.
Hearing problems 40 times more common.
Upto 2/3rd
ofpersons with ID have comorbid mental illness.
As the severity increases,risk for mental illness increases.
Disruptive and conduct disorders are common in mild cases.
Autistic disorders common in severely retarded individuals.
Schizophrenia over-represented -4.4% in ID vs 0.4% in general
population.
The prevalence of psychiatric disorders in individuals with ID
is estimated to be in between 30%-60%.
48.
Possible Causes ofIncreased
Vulnerability to Mental Disorders in
Persons with Intellectual Disability
Neuropathological processes responsible for intellectual
disability may also cause or increase the risk for mental
illness.
Increased likelihood of loss and separation,particularly in
out-of-home placements.
Communication deficits may predispose to emotional/
behavioral disturbance.
49.
Vulnerability toexploitation and abuse by others.
Inadequate coping skills.
Family stress may be heightened in the presence of a
child with developmental disability.
Limited network of social relationships.
Reduced opportunities for the development and exercise
of recreational and occupational skills.
50.
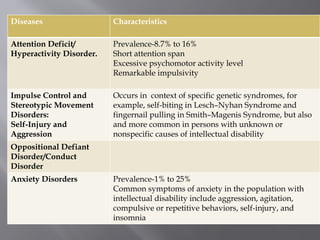
Diseases Characteristics
Attention Deficit/
HyperactivityDisorder.
Prevalence-8.7% to 16%
Short attention span
Excessive psychomotor activity level
Remarkable impulsivity
Impulse Control and
Stereotypic Movement
Disorders:
Self-Injury and
Aggression
Occurs in context of specific genetic syndromes, for
example, self-biting in Lesch–Nyhan Syndrome and
fingernail pulling in Smith–Magenis Syndrome, but also
and more common in persons with unknown or
nonspecific causes of intellectual disability
Oppositional Defiant
Disorder/Conduct
Disorder
Anxiety Disorders Prevalence-1% to 25%
Common symptoms of anxiety in the population with
intellectual disability include aggression, agitation,
compulsive or repetitive behaviors, self-injury, and
insomnia
51.
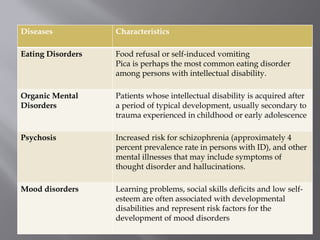
Diseases Characteristics
Eating DisordersFood refusal or self-induced vomiting
Pica is perhaps the most common eating disorder
among persons with intellectual disability.
Organic Mental
Disorders
Patients whose intellectual disability is acquired after
a period of typical development, usually secondary to
trauma experienced in childhood or early adolescence
Psychosis Increased risk for schizophrenia (approximately 4
percent prevalence rate in persons with ID), and other
mental illnesses that may include symptoms of
thought disorder and hallucinations.
Mood disorders Learning problems, social skills deficits and low self-
esteem are often associated with developmental
disabilities and represent risk factors for the
development of mood disorders
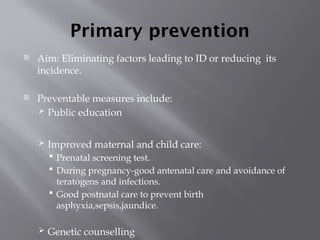
Primary prevention
Aim:Eliminating factors leading to ID or reducing its
incidence.
Preventable measures include:
Public education
Improved maternal and child care:
Prenatal screening test.
During pregnancy-good antenatal care and avoidance of
teratogens and infections.
Good postnatal care to prevent birth
asphyxia,sepsis,jaundice.
Genetic counselling
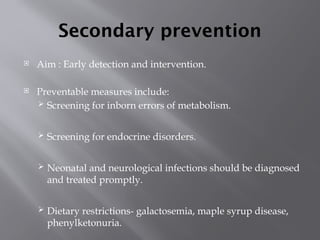
54.
Secondary prevention
Aim: Early detection and intervention.
Preventable measures include:
Screening for inborn errors of metabolism.
Screening for endocrine disorders.
Neonatal and neurological infections should be diagnosed
and treated promptly.
Dietary restrictions- galactosemia, maple syrup disease,
phenylketonuria.
55.
Tertiary preventions
Aim:minimize the complications or sequelae resulting
from ID
Measures include:
Parental counselling.
Management of emotional and behavioural problems.
Rehabilitation.
Special education facilities.
56.
CLINICAL ASSESSMENT
Clinical History
Prenatal exposures (alcohol, infections, etc.)
Birth history
CNS infection, traumatic brain injury
Developmental regression
Focal neurological findings, hypertonia, hypotonia,
or ataxia
Extra-CNS malformations and medical issues
Visual impairment or hearing loss
57.
Family Pedigree (Three-Generation)
Relatives with learning problems, psychiatric
disorders, intellectual disability, abnormal
brain imaging.
Consanguinity
58.
Physical Examination
Assessmentof major and minor physical anomalies
including facial features and skin findings
Growth and physical development
Head circumference compared to norms (congenital
versus “acquired” microcephaly/macrocephaly)
Growth trajectory (comparison with earlier
measures)
Description of facial features (micrognathia,
hypertelorism, thin upper lip)
Complete neurological examination
Skin examination for café-au-lait and other
birthmarks
Documentation of behavioral phenotype
59.
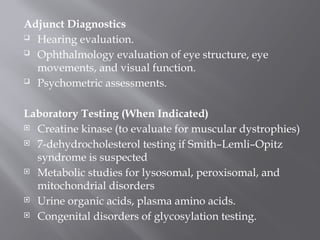
Adjunct Diagnostics
Hearingevaluation.
Ophthalmology evaluation of eye structure, eye
movements, and visual function.
Psychometric assessments.
Laboratory Testing (When Indicated)
Creatine kinase (to evaluate for muscular dystrophies)
7-dehydrocholesterol testing if Smith–Lemli–Opitz
syndrome is suspected
Metabolic studies for lysosomal, peroxisomal, and
mitochondrial disorders
Urine organic acids, plasma amino acids.
Congenital disorders of glycosylation testing.
60.
Genetic Testing (WhenIndicated)
Chromosomal microarray
Fragile X testing
DNA sequencing (single gene, gene panel, whole exome)
DNA methylation testing if Prader–Willi or Angelman
syndromes are suspected
Imaging
Structural brain magnetic resonance imaging [MRI]
Functional brain MRI [fMRI] (still largely research-based)
Diffusion tensor brain MRI [DTI]
Other Studies
Muscle biopsy for suspected mitochondrial disease (or
muscular dystrophy)
61.
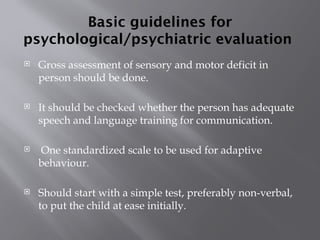
Basic guidelines for
psychological/psychiatricevaluation
Gross assessment of sensory and motor deficit in
person should be done.
It should be checked whether the person has adequate
speech and language training for communication.
One standardized scale to be used for adaptive
behaviour.
Should start with a simple test, preferably non-verbal,
to put the child at ease initially.
62.
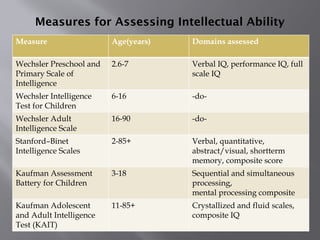
Measures for AssessingIntellectual Ability
Measure Age(years) Domains assessed
Wechsler Preschool and
Primary Scale of
Intelligence
2.6-7 Verbal IQ, performance IQ, full
scale IQ
Wechsler Intelligence
Test for Children
6-16 -do-
Wechsler Adult
Intelligence Scale
16-90 -do-
Stanford–Binet
Intelligence Scales
2-85+ Verbal, quantitative,
abstract/visual, shortterm
memory, composite score
Kaufman Assessment
Battery for Children
3-18 Sequential and simultaneous
processing,
mental processing composite
Kaufman Adolescent
and Adult Intelligence
Test (KAIT)
11-85+ Crystallized and fluid scales,
composite IQ
63.
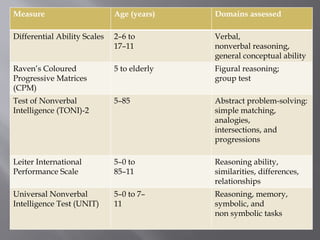
Measure Age (years)Domains assessed
Differential Ability Scales 2–6 to
17–11
Verbal,
nonverbal reasoning,
general conceptual ability
Raven’s Coloured
Progressive Matrices
(CPM)
5 to elderly Figural reasoning;
group test
Test of Nonverbal
Intelligence (TONI)-2
5–85 Abstract problem-solving:
simple matching,
analogies,
intersections, and
progressions
Leiter International
Performance Scale
5–0 to
85–11
Reasoning ability,
similarities, differences,
relationships
Universal Nonverbal
Intelligence Test (UNIT)
5–0 to 7–
11
Reasoning, memory,
symbolic, and
non symbolic tasks
64.
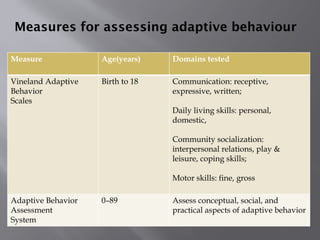
Measures for assessingadaptive behaviour
Measure Age(years) Domains tested
Vineland Adaptive
Behavior
Scales
Birth to 18 Communication: receptive,
expressive, written;
Daily living skills: personal,
domestic,
Community socialization:
interpersonal relations, play &
leisure, coping skills;
Motor skills: fine, gross
Adaptive Behavior
Assessment
System
0–89 Assess conceptual, social, and
practical aspects of adaptive behavior
65.
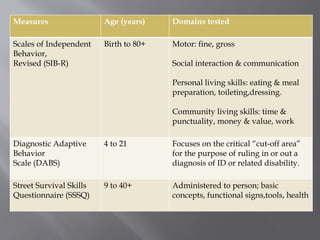
Measures Age (years)Domains tested
Scales of Independent
Behavior,
Revised (SIB-R)
Birth to 80+ Motor: fine, gross
Social interaction & communication
Personal living skills: eating & meal
preparation, toileting,dressing.
Community living skills: time &
punctuality, money & value, work
Diagnostic Adaptive
Behavior
Scale (DABS)
4 to 21 Focuses on the critical “cut-off area”
for the purpose of ruling in or out a
diagnosis of ID or related disability.
Street Survival Skills
Questionnaire (SSSQ)
9 to 40+ Administered to person; basic
concepts, functional signs,tools, health
66.
Intellectual assessment toolsused
in India
Verbal test:
Binet Kamat test.
Binet Kulshresta test.
Malin’s intelligence test for Indian children.
Non-verbal and performance test:
Developmental screening test.
Raven’s progressive matrices.
Seguin form board test.
Gassel’s drawing test.
Malin’s intelligence scale for Indian children performance.
Alexander pass along test.
Draw –A-Man test.
Koch’s block design test
Enhancing self image
Acceptance of ID child in the family and
society.
Availability of proper facilities for learning and
developing skills and later suitable jobs.
69.
Management of psychiatriccomorbidities
Intellectual disability is a multidisciplinary problem, and
optimal treatment is multimodal.
A treatment plan will include
psychoeducational,
psychotherapeutic, and
psychopharmacological interventions
70.
Psychotherapy
Specific psychotherapeuticapproaches that have been
shown to be effective include behavioral (in particular,
applied behavior analysis models), cognitive–
behavioral, psycho-educational, and skills training
(e.g., coping skills, social skills).
Behavioral therapies are demonstrably effective in
managing many maladaptive behaviors, particularly
aggression and self-injury, in persons with ID.
Interventions that should be considered include
environmental modifications, caregiver education, and
applied behavior analysis (ABA).
71.
Pharmacotherapy
Drugs shouldonly be used for specific indications like
psychosis, depression, anxiety, ADHD.
ID patients are more sensitive to side effects and prone
to drug toxicity.
Responsive to lower doses of psychotropics-
Golden rule: start low, go slow.
72.
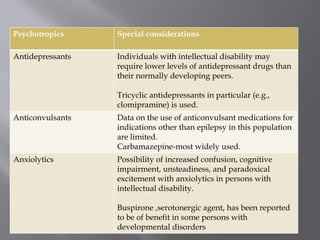
Psychotropics Special considerations
AntidepressantsIndividuals with intellectual disability may
require lower levels of antidepressant drugs than
their normally developing peers.
Tricyclic antidepressants in particular (e.g.,
clomipramine) is used.
Anticonvulsants Data on the use of anticonvulsant medications for
indications other than epilepsy in this population
are limited.
Carbamazepine-most widely used.
Anxiolytics Possibility of increased confusion, cognitive
impairment, unsteadiness, and paradoxical
excitement with anxiolytics in persons with
intellectual disability.
Buspirone ,serotonergic agent, has been reported
to be of benefit in some persons with
developmental disorders
73.
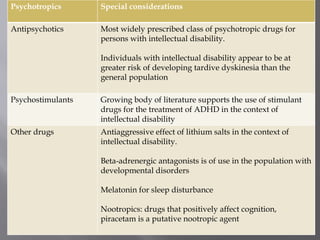
Psychotropics Special considerations
AntipsychoticsMost widely prescribed class of psychotropic drugs for
persons with intellectual disability.
Individuals with intellectual disability appear to be at
greater risk of developing tardive dyskinesia than the
general population
Psychostimulants Growing body of literature supports the use of stimulant
drugs for the treatment of ADHD in the context of
intellectual disability
Other drugs Antiaggressive effect of lithium salts in the context of
intellectual disability.
Beta-adrenergic antagonists is of use in the population with
developmental disorders
Melatonin for sleep disturbance
Nootropics: drugs that positively affect cognition,
piracetam is a putative nootropic agent
74.
Skill training
Givenby:
Special schools.
Vocational training centres.
Child guidance clinic in general hospital.
Steps :
Training activity should be divided into small steps
and demonstrated properly.
Repeated training in each activity.
Train regularly and systematically.
75.
Parent counselling
Itis an important step in management of ID
patients.
Stages of counselling are:
Imparting information regarding the condition of the
ID child.
Helping the parent to develop right attitude towards
their disabled child.
Creating awareness in the parent regarding their role
in training their child.
76.
Rehabilitation
Depending upontheir learning potential,
prevocational and vocational training needs to
be provided.
Vocational services include:
Counselling of the trainers and their families.
Supported employment including job placements.
77.
Role of psychiatrist
As a diagnostician, therapist and researcher.
Intermediary and coordinator between staff
and physicians in other specialities.
As a consultant at various special schools or
institute for ID.
Rehabilitation services.
The NATIONALTRUST works for the welfare
of persons with any of the four disabilities:
Autism.
Cerebral palsy.
Mental retardation.
Multiple disabilities.
80.
Samarth scheme:
Itcovers all the four disabilities under the national trust.
It’s a centre based scheme (july 2005) for residential
services to these four groups.
Activities include- early intervention, special education,
prevocational and vocational training, employment
oriented training, recreation sports, etc.
Niramaya:
This is a health insurance scheme to provide affordable
health insurance to these 4 groups.
Health insurance is provided upto Rs. 1.0 lakh.
81.
Government sanctioned organizationsworking for special
need children and adults in Assam
Dhule Regional Physical Development Association
ASCENT
Disabled Person Welfare & Rehabilation Trust
Shishu Sarothi Spastic Society of Assam
Swabalambi
Ashadeep
Guwahati Mental Welfare Society
Prerona Spastic Society of Jorhat
Kachajuli Physically Handicapped School and Training Centre
Bikalanga Kalyan Kendra"TELAHI"
Gram Vikas Parishad
Global Health and Educatin Centre(GHEC)
82.
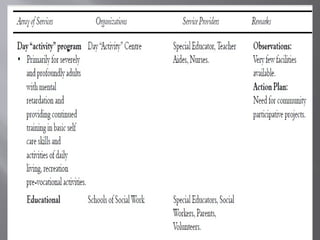
Persons with disabilityact,1995
With the implementation of Persons with
Disabilities Act, 1995, an array of services for
persons with intellectual disability is available.
Salient features:
The types of disabilities have been increased from
existing 7 to 21.
Effective measures have been taken to ensure that
the persons with disabilities enjoy their rights
equally with others.
Additional benefits such as reservation in higher
education, government jobs, reservation in allocation
of land, poverty alleviation schemes etc. have been
provided for persons with benchmark disabilities
and those with high support needs
93.
Every childwith benchmark disability between the age
group of 6 and 18 years shall have the right to free
education.
Government funded educational institutions as well as
the government recognized institutions will have to
provide inclusive education to the children with
disabilities.
Reservation in vacancies in government establishments
has been increased from 3% to 4% for certain persons
or class of persons with benchmark disability
94.
Disability certificate
Eligibilitycriteria:
Disability of 40% and above
Bonafide citizen of india
%of disability= 110- IQ score
Issued by:
Psychiatrist
Paediatrician
Clinical psychologist
National legal servicesauthority
scheme,2010
Mentally retarded persons are not mentally ill persons.
Right to education.
Laws for prevention of exploitation and abuse.
Legal services for owing and inheriting properties and to
have financial rights.
Appointment of guardians under the National Trust
Act,1999.
Creating awareness campaigns among other school
children.
Awareness camps for educating the family members.
Awareness programmes for the general public.
Sensitization programme for juidicial officers and lawyers.
Conclusion
The highprevalence and persistence of psychopathology
among children and adolescents with ID, when combined
with existing knowledge regarding risk factors and
possible underlying mechanisms, open up the possibility
of developing more preventative approaches.
Future research and practice hold out the possibility of
advances on three fronts:
furthering our understanding of the biological bases of ID;
strengthening the evidence-base for specific interventions;
developing a more preventative approach to addressing
psychopathology in children and adolescents with ID.
99.
Bibliography
H.K.Bryan etal.Intellectual disability: Benjamin J.
Sadock, Virginia A Sadock Pedro Ruiz.
COMPREHENSIVE TEXTBOOK OF PSYCHIATRY: 10th
edition.
Association, American Psychiatric (2013). Diagnostic and
statistical manual of mental disorders:DSM5. (5th ed.).
Washington, D.C.: American Psychiatric Association. p.
34.
31.1 intellectual disability: Kaplan and Sadock’s
Synopsis of Psychiatry:11th
edition. Page-1118-37.
100.
Stewart Einfeldand Eric Emerson. Intellectual
Disability: Michael Rutter et al,editors. Rutter’s Child
and Adolescent Psychiatry.
Mental retardation-a manual for psychologists-
NIMH,Ministry of Social Justice,Govt of India
http://
pib.nic.in/newsite/PrintRelease.aspx?relid=155592
http://www.rehabcouncil.nic.in/writereaddata/mr.pdf
http://www.udaan.org/parivaar/india.html#ASSAM







![Genetic Testing (When Indicated)
Chromosomal microarray
Fragile X testing
DNA sequencing (single gene, gene panel, whole exome)
DNA methylation testing if Prader–Willi or Angelman
syndromes are suspected
Imaging
Structural brain magnetic resonance imaging [MRI]
Functional brain MRI [fMRI] (still largely research-based)
Diffusion tensor brain MRI [DTI]
Other Studies
Muscle biopsy for suspected mitochondrial disease (or
muscular dystrophy)](https://image.slidesharecdn.com/intellectualdisability-250904120031-cb0bbe1d/85/An-overview-of-intellectual-disability-60-320.jpg)






















![MENTAL_RETARDATION[1] by emma MAGOMA.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mentalretardation1byemmamagoma-251014190048-74e29c31-thumbnail.jpg?width=640&height=640&fit=bounds)























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




