This document defines and describes infective endocarditis. Key points include:
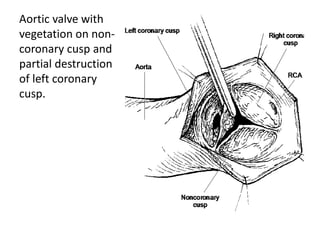
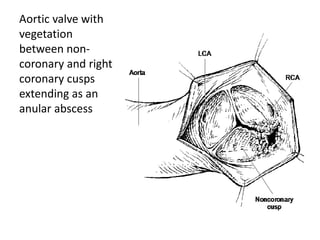
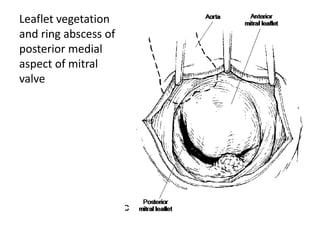
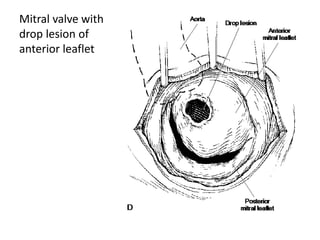
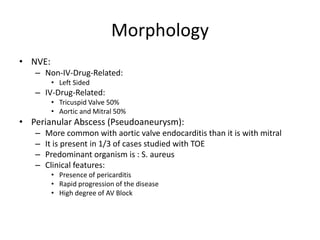
- Infective endocarditis involves infection of the heart valves or structures, most commonly the valves. This can lead to valvular dysfunction, sepsis, or embolism.
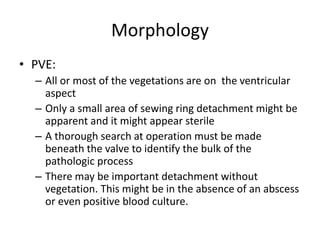
- The infection involves bacterial, viral, or fungal invasion of the endocardium and formation of vegetations on the valves or endocardium.
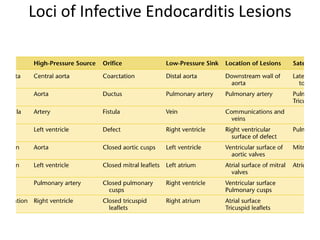
- Risk factors include underlying heart conditions, IV drug use, dental procedures, and indwelling catheters. The aortic and mitral valves are most commonly involved.
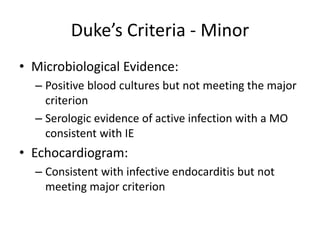
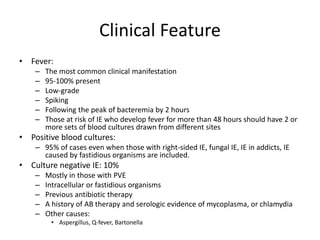
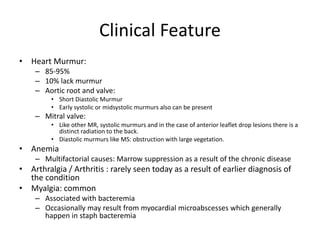
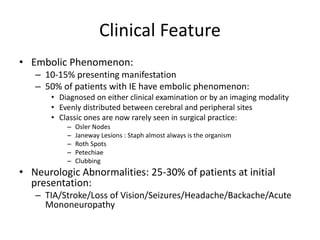
- Symptoms may include fever, heart murmur, embolic phenomena, and heart failure. Diagnosis






































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















