Downloaded 1,083 times


























![Erectile Dysfunction [Dr. Edmond Wong]](https://image.slidesharecdn.com/ededmond-140716212750-phpapp02/85/Erectile-Dysfunction-Dr-Edmond-Wong-172-320.jpg)

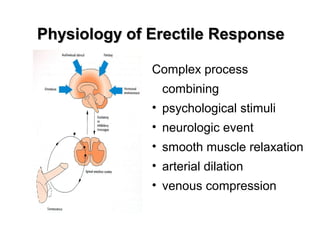
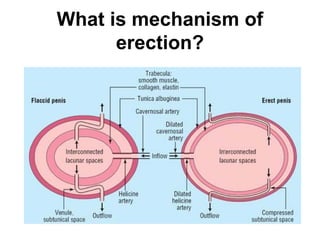
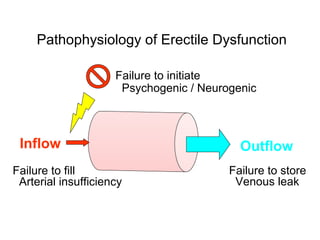
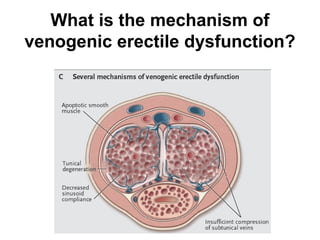
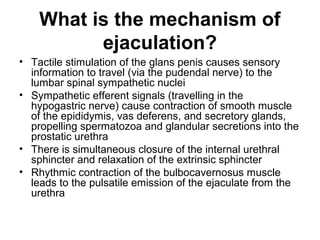
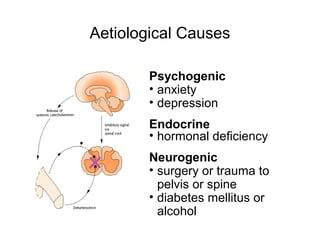
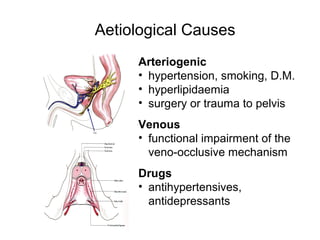
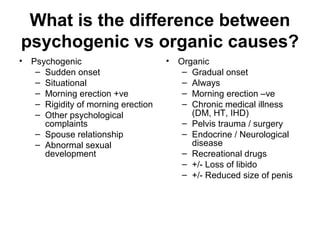
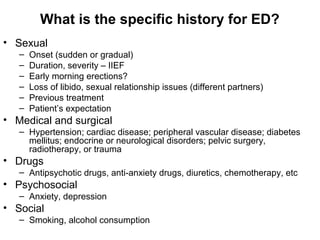
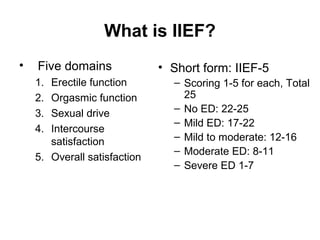
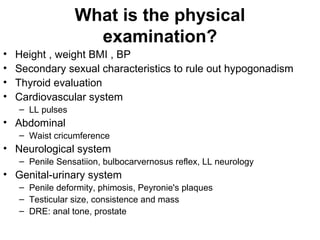
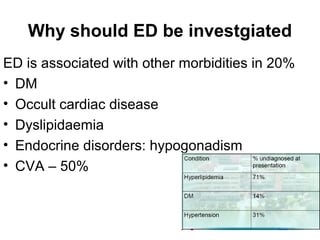
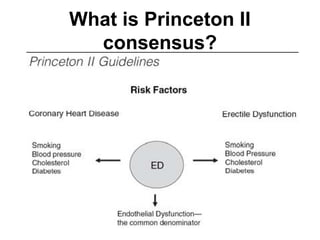
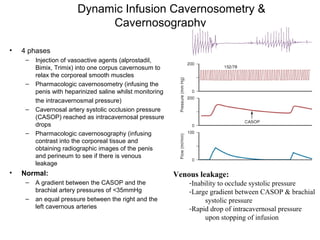
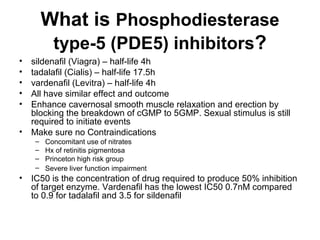
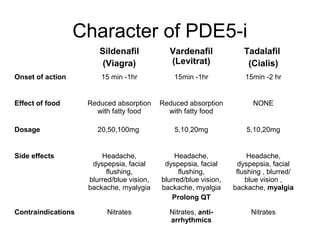
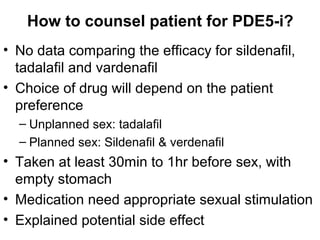
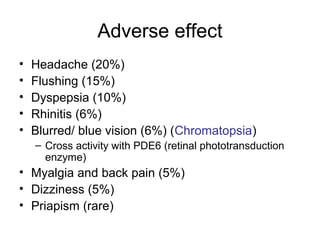
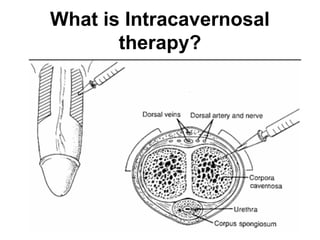
This document discusses male sexual dysfunction and erectile dysfunction (ED). It defines ED and provides prevalence data, noting that the risk of ED increases with age. It describes the anatomy involved in erection, ejaculation, and the arterial and venous blood supply of the penis. The mechanisms and phases of erection are explained. Common risk factors, causes, and medications associated with ED are listed. Methods for diagnosing ED including history, physical exam, the International Index of Erectile Function (IIEF), and potential tests like nocturnal penile tumescence monitoring and duplex ultrasound are outlined.















![Infertility [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/infertilityedmond-140716214842-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




![Benign Prostatic Hyperplasia BPH [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/bphedmond-140716213908-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)














































![Human Renal Transplantation [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/humanrenaltransplantationedmond-140716214736-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Emergency in Urology [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/emergencyuroedmond-140716213857-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Neurogenic bladder [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/neurogenicbladderedmond-140716213757-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Muscle invasive bladder Cancer [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/muscleinvasivebladdertumoredmond-140716213247-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Incontinence & Female Urology [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/incontinencefemaleedmond-140716213134-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Urinary Stone Management [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/stonemanagementedmond-140716213042-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Paediatric Urology [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/paeduroedmond-140716213023-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Bladder Cancer NMIBC [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/non-muscleinvasivebladdertumoredmond-140716212950-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Urology New Technology and Imaging [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/newtechimagingedmond-140716212943-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Urology infection [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/urologyinfectionedmond-140716212859-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Urinary Diversion after cystectomy [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/urinarydiversionedmond-140716212817-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Upper Tract Transitional Cell Carcinoma [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/uppertracttccedmond-140716212806-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Testicular ca [edmond]](https://cdn.slidesharecdn.com/ss_thumbnails/testicularcaedmond-130318091757-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Ca penis [edmond]](https://cdn.slidesharecdn.com/ss_thumbnails/capenisedmond-130318091738-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Ca kidney [edmond]](https://cdn.slidesharecdn.com/ss_thumbnails/cakidneyedmond-130318091659-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
![Ca prostate [edmond]](https://cdn.slidesharecdn.com/ss_thumbnails/caprostateedmond-130318091345-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



















