Downloaded 409 times

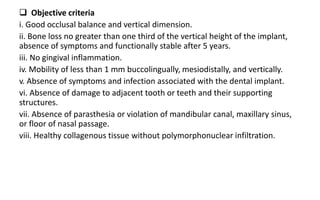
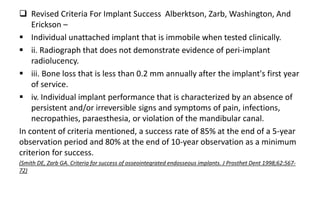
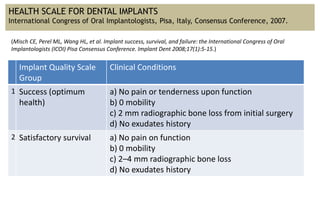
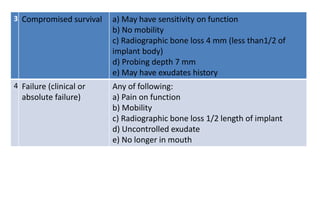




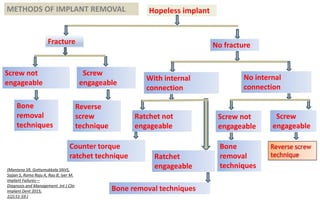
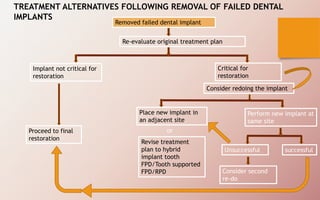


The document discusses the various aspects of dental implant failure and treatment, including criteria for success, classifications of implant failure, risk factors, and management strategies. It emphasizes the importance of assessing clinical and radiographic conditions, identifying issues such as biological, mechanical, and iatrogenic failures, as well as the significance of host factors like systemic diseases and habits. The document outlines methods for diagnosis, management options for failing implants, and the need for appropriate implant placement and maintenance to improve outcomes.














































































