Downloaded 216 times
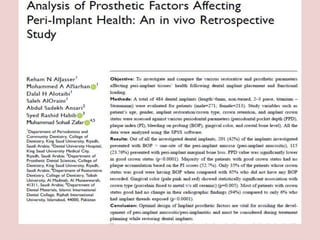
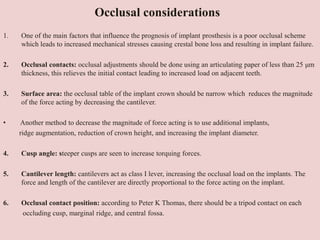
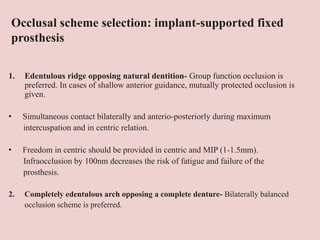

The document discusses prosthetic considerations for implant patients, emphasizing the importance of proper treatment planning, peri-implant tissue health, and factors influencing implant success. It highlights the relationship between implant design, patient anatomy, and prosthetic approaches tailored to bone conditions, as well as the impact of occlusal forces and the importance of maintaining oral hygiene. Key considerations include ensuring adequate bone density, appropriate implant positioning, and the management of loading protocols to optimize long-term outcomes.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





