
Download to read offline



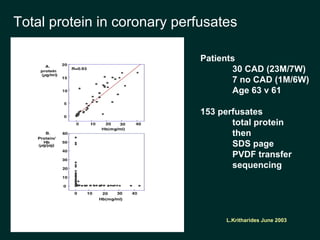

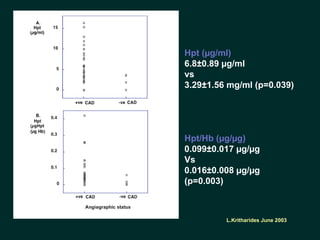
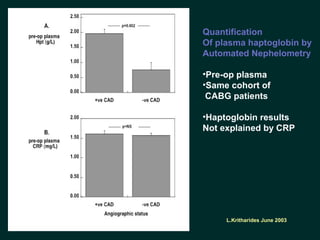
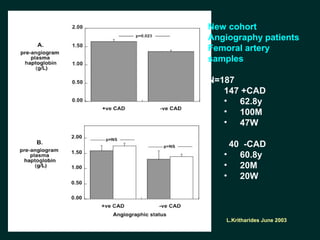
This document discusses a study aimed at identifying new biomarkers for coronary artery disease. The researcher hypothesized that molecules which more readily leave the artery wall during perfusion would also more readily leave in vivo, and that differences in proteins eluted from atherosclerotic versus non-atherosclerotic arteries could indicate different biomarkers. The study involved perfusing arteries prior to bypass surgery and analyzing perfusate proteins. One protein, haptoglobin, was higher in perfusates and blood samples from patients with coronary artery disease versus those without. This proof-of-principle study suggests coordinating perfusion strategies with proteomics may help identify new disease-specific arterial markers.

























































![Interpretation of Clinical Lab Data [CARDIAC] for newbies.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/interpretationofclinicallabdatacardiacfornewbies-230518071258-e33c3626-thumbnail.jpg?width=640&height=640&fit=bounds)
















































