


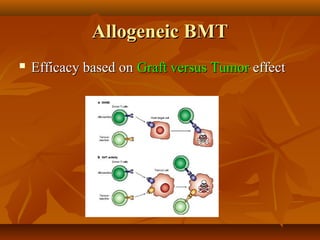

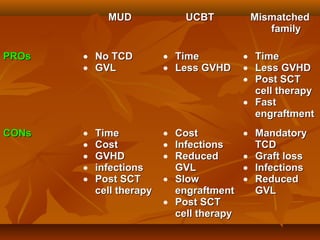
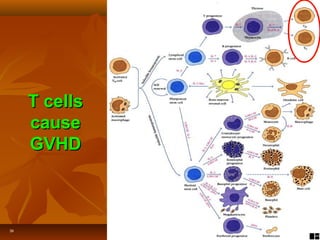
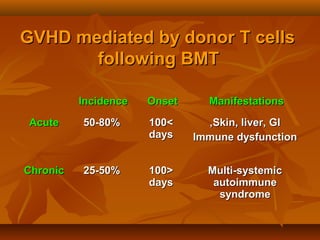




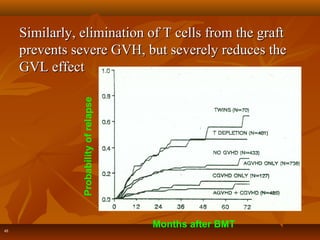
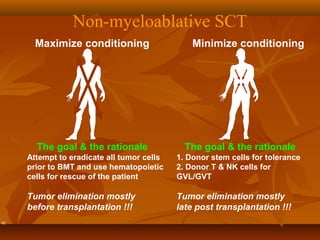

Bone marrow transplantation involves harvesting stem cells from either the patient (autologous) or a donor (allogeneic) and administering high-dose chemotherapy to eliminate malignant or damaged bone marrow cells. Allogeneic transplants can provide a graft-versus-tumor effect from donor immune cells attacking cancer cells, but also risk graft-versus-host disease as donor cells may attack patient tissues. The choice of donor, degree of tissue matching, and immuno-modulation of the graft influence efficacy and complications like relapse and GVHD. Further research aims to maximize the graft-versus-tumor effect while minimizing graft rejection and side effects.






















































































