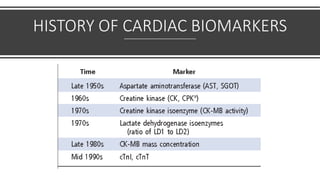
Cardiac biomarkers are proteins released when heart muscle is damaged and can help diagnose and manage cardiovascular diseases. Commonly used biomarkers include cardiac troponins and natriuretic peptides. Troponins indicate heart muscle injury while natriuretic peptides reflect heart failure. High sensitivity troponin assays can detect very low levels and aid early diagnosis of heart attacks. Emerging biomarkers of inflammation like interleukin-6 may also provide prognostic information. Biomarkers are detected at different times after injury and combining their measurements over time can improve the assessment of patients with suspected cardiovascular issues.