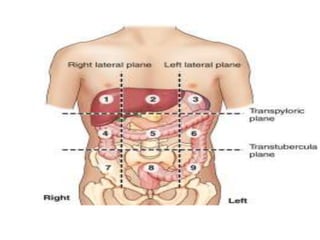
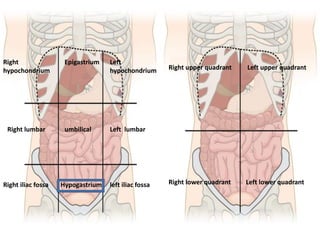
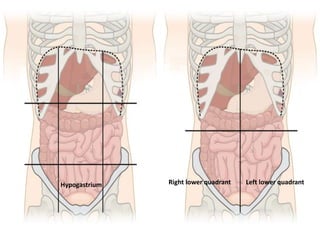
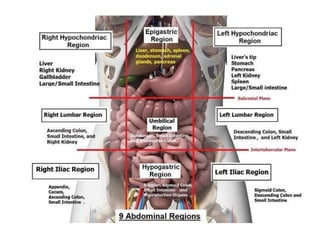
This document provides guidance on evaluating a patient presenting with an abdominal lump. It outlines taking a thorough history including demographics, present complaints, past medical history, and family history. A comprehensive physical exam of the abdomen is described including inspection, palpation, percussion, and auscultation. Differential diagnoses are discussed depending on the location of the lump in the hypogastric region. Investigations guided by history and exam such as ultrasound and organ-specific tests are recommended to determine the nature and origin of the lump.