Topic: Revision ofcase of
Right Upper Quadrant
Abdominal Lump
-Dr. Rana M. Rajneesh
Head of Unit 3
Deptt. Of Surgery
5.
A sequential approachto a patient complaining about abdominal lump
-
● Extracting relevant history
● Thorough clinical examination
● Correct diagnosis by conducting investigations guided by above
history & examination
● Offering adequate treatment
6.
History
● Demographic data-
○ Age
○ Gender
○ Occupation
○ Address
○ Socio economic status
○ Date of admission
○ Date of examination
○ Bed no.
7.
● Presenting complaints-
○ abdominal lump: Mode of onset (Whether appeared spontaneously or after
trauma/surgery), duration, site, approx size, progression/regression, any
association with meals/posture/straining/trauma, whether disappears
spontaneously
○ pain: site, onset, duration, character, radiation/migration/referred, any
relieving /aggravating factors
● Other associated complaints -
○ nausea/vomiting: character, amount, frequency, content (hematemesis),
○ relieving/aggravating factors, altered bowel habit: diarrhea, constipation,
obstipation, flatulent dyspepsia etc
○ melaena/hematochezia
○ jaundice: onset, duration, progression etc.
8.
● Past &personal history:
○ Comorbidity/treatments- medical or surgical
○ Sleep-wake cycle/ eating habits/ appetite/ bladder & bowel habits/
substance abuse
○ Family/ menstrual & obstetric history
● Parietal vsintra abdominal swelling
If the swelling is parietal the swelling will become more prominent (Intra-
abdominal swelling becomes less prominent) when the abdominal muscles
are made taut and will be freely movable over the taut muscle.
If the swelling is parietal but fixed to the abdominal muscle the swelling will
not be movable when the muscles are made taut
Another differentiating point is that if the swelling moves vertically with
respiration it is obviously an intra-abdominal swelling.
13.
● Percussion:
○ Techniquefor lump
○ Technique for evaluation of ascites
○ Span of organomegaly
○ Solid lump-dull (superficial), resonant(coils of bowel overlying)
● Auscultation:
○ Bowel sounds
○ Abnormal sounds (bruit, hums)
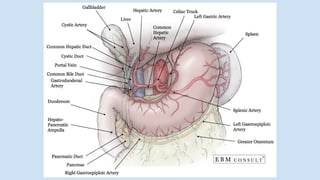
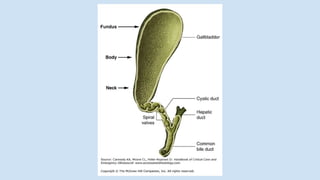
● Gallbladder: benign-smooth globular lump, upper margin
not defined, movement with respiration
○ Acute cholecystitis (Murphy’s sign: At the height of inspiration when
the inflamed gallbladder impinges on the thumb there will be a catch
in breath and patient will wince with pain. The Murphy’s sign is said to
be positive)
○ Mucocele
○ Empyema with stone impaction neck
○ Porcelain gallbladder: Extensive calcium encrustation of gallbladder.
‘Porcelain’ refers to bluish discoloration and brittle consistency.
○ Carcinoma gallbladder




















![Right hypochondrium lump[1]](https://cdn.slidesharecdn.com/ss_thumbnails/righthypochondriumlump1-210330201334-thumbnail.jpg?width=640&height=640&fit=bounds)
























![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)


