

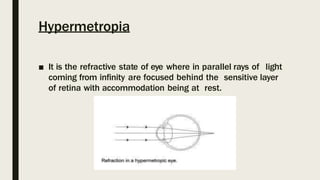


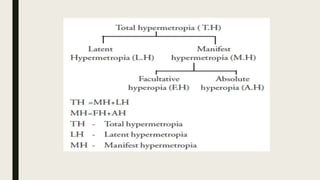


Hypermetropia, also known as farsightedness, is a refractive error where the eye focuses light behind the retina when the eye is at rest. There are several types of hypermetropia including axial, refractive, index, curvature, and anterior chamber hypermetropia. Hypermetropia can also be classified as simple, pathological, or functional based on physiological and anatomical factors. It can be further broken down into total, manifest, latent, and facultative hypermetropia depending on whether it can be corrected with accommodation. Treatment options include spectacle correction with convex lenses, contact lenses, and refractive surgery procedures like LASIK.























































































