Download to read offline

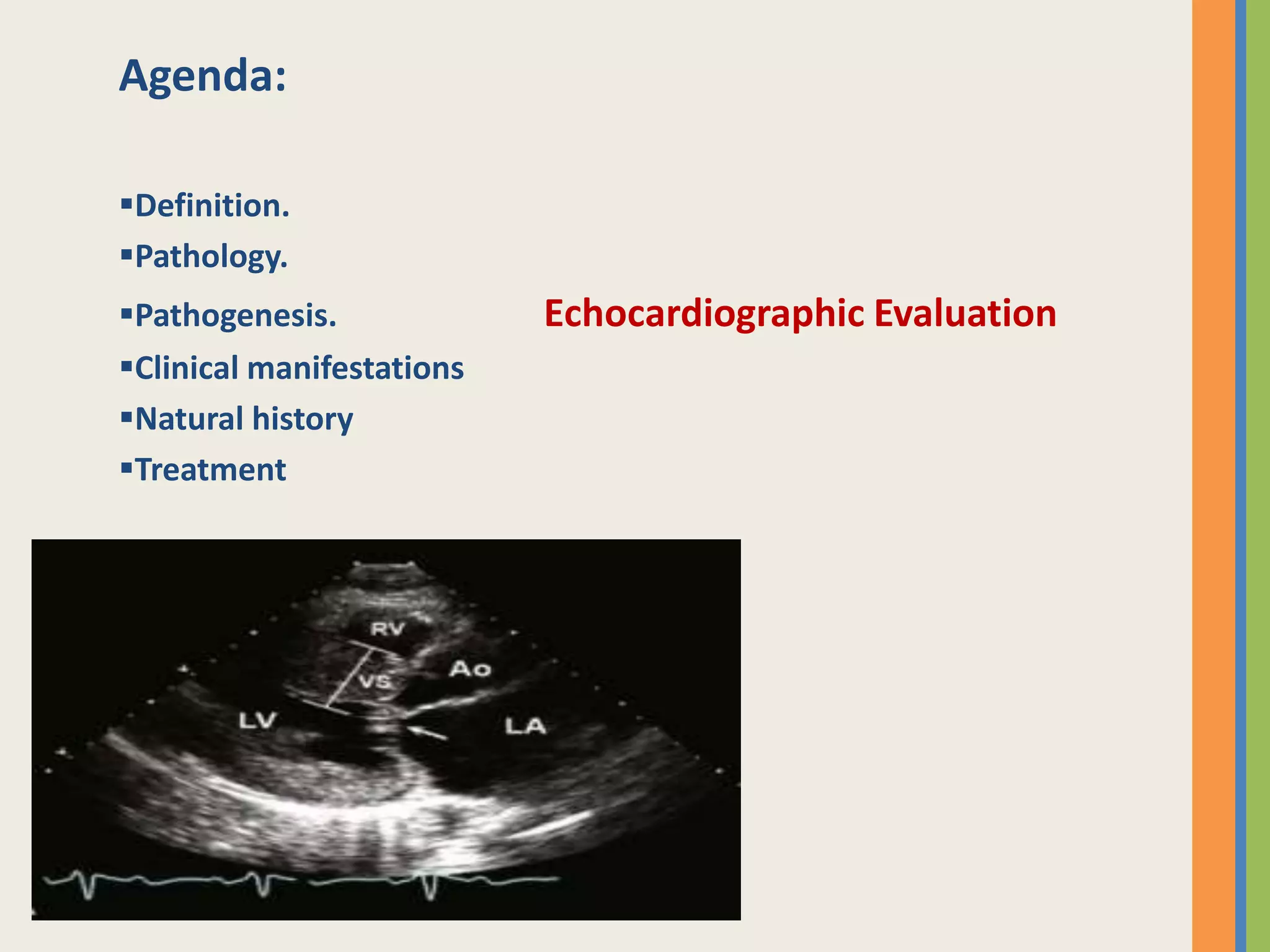










































This document summarizes hypertrophic cardiomyopathy (HCM), beginning with its pathology and pathogenesis. HCM causes thickening of the ventricular walls asymmetrically, most commonly affecting the interventricular septum. The main pathophysiological mechanisms include dynamic left ventricular outflow tract obstruction, mitral regurgitation, diastolic dysfunction, myocardial ischemia, and cardiac arrhythmias. Clinical manifestations range from no symptoms to dyspnea, fatigue, syncope, and sudden cardiac death. Diagnosis is made primarily via echocardiogram. Treatment involves medications, septal reduction procedures, or implantable cardioverter-defibrillators depending on symptoms and risk factors. Prognosis depends on factors like degree of









































































