Downloaded 929 times


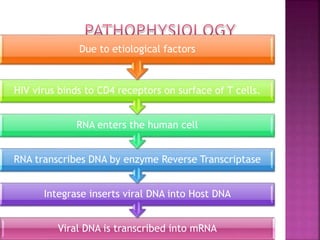
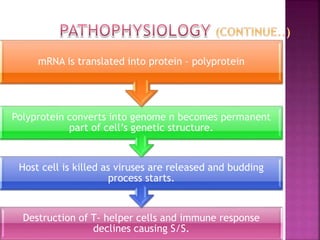
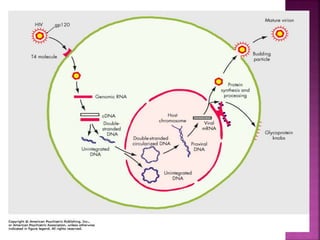
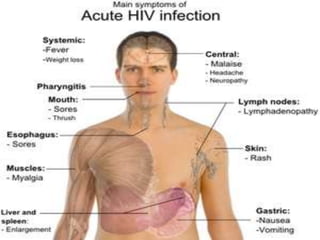


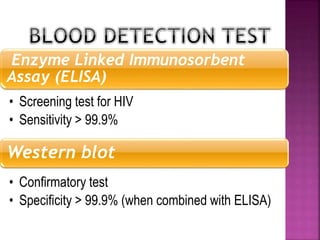
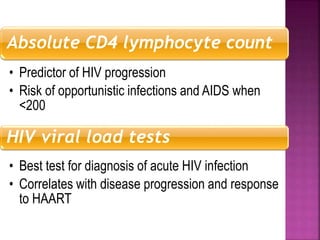
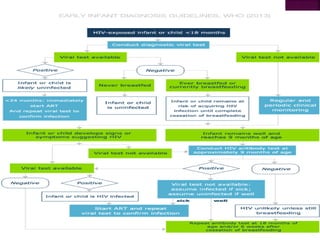


The document discusses HIV/AIDS in children. It defines HIV as a virus that infects and weakens the immune system, and AIDS as the syndrome that occurs when the immune system is severely damaged by HIV. HIV is usually transmitted from mother to child during pregnancy, childbirth or breastfeeding. Children with HIV may show no symptoms for years but can eventually develop infections like pneumonia or develop AIDS. There are screening tests to detect HIV in children but no vaccine or cure currently exists. Antiretroviral treatment can slow disease progression.





























































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)