Downloaded 53 times


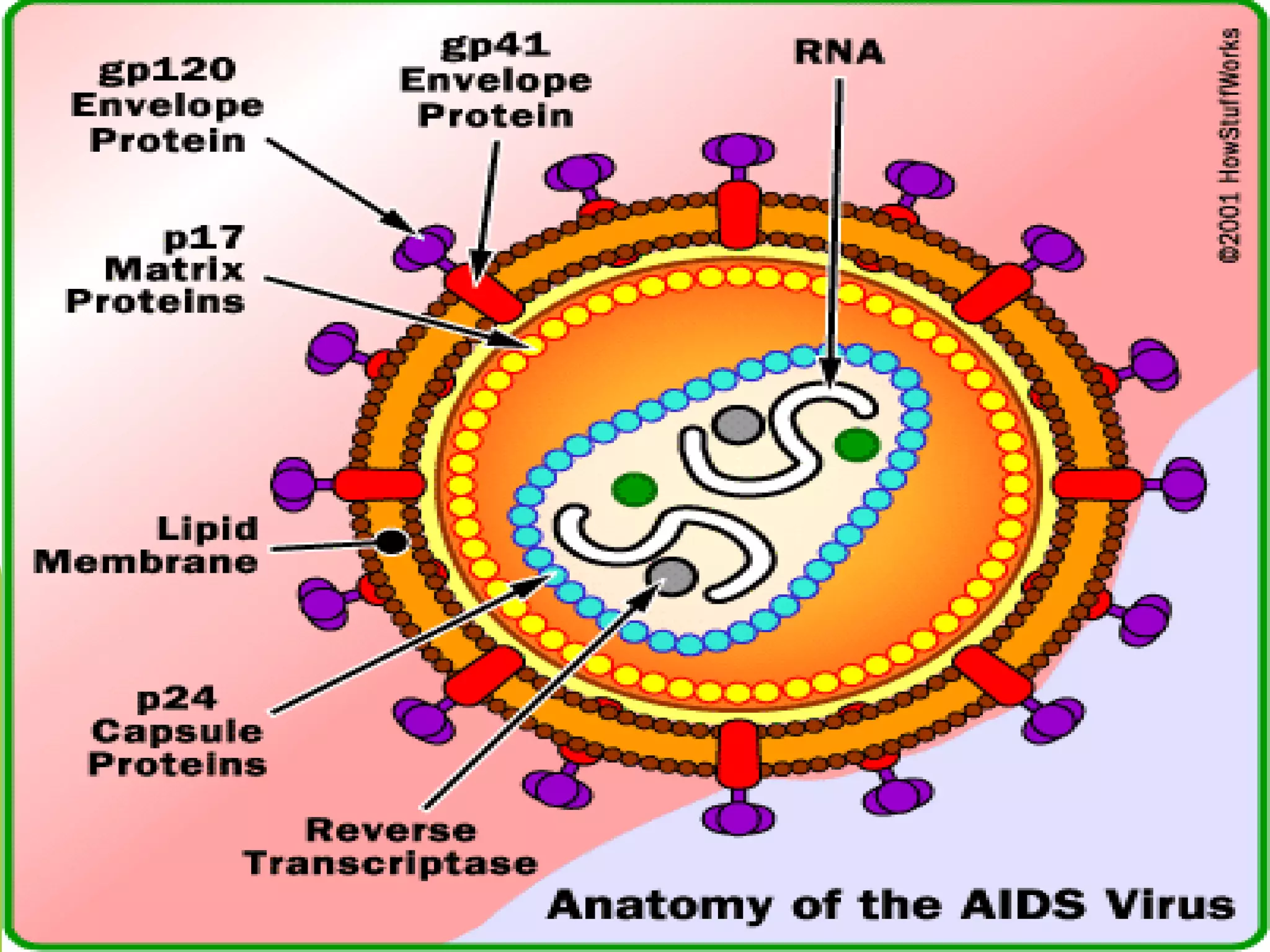





















This document discusses Acquired Immunodeficiency Syndrome (AIDS) in children. It defines AIDS as a fatal illness caused by the human immunodeficiency virus (HIV) that breaks down the body's immune system. The document notes that in 2002, an estimated 800,000 children under 15 were newly infected with HIV worldwide and 610,000 children died of AIDS. It provides classifications for HIV infection in children and discusses routes of transmission, clinical features, diagnostic evaluations, common conditions, complications, and nursing management of pediatric AIDS.
















































































