Downloaded 75 times


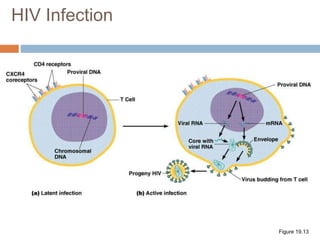
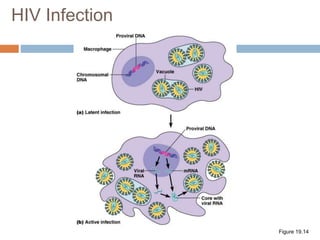
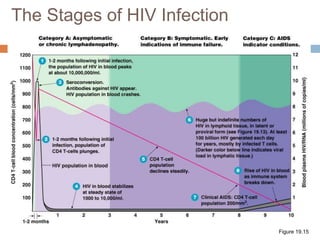
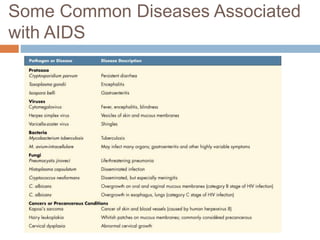




HIV is a retrovirus that causes AIDS by destroying CD4+ T cells. It is transmitted through bodily fluids and can be occupational hazard for surgeons. Universal precautions like proper protective equipment and disposal of contaminated waste are important to prevent transmission. Current antiretroviral therapy uses combination of three or more drugs like nucleoside analogs that inhibit reverse transcriptase and protease inhibitors. This effectively suppresses the virus and prevents opportunistic infections associated with AIDS.









































![HUMAN_IMMUNODEFICIENCY_VIRUS[1]. pptx](https://cdn.slidesharecdn.com/ss_thumbnails/humanimmunodeficiencyvirus1-250922103632-2012e6ee-thumbnail.jpg?width=640&height=640&fit=bounds)














![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










