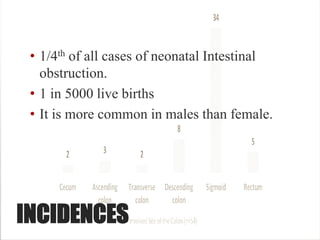
This document provides an overview of Hirschsprung disease including:
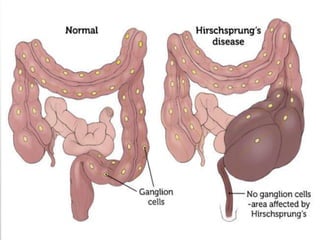
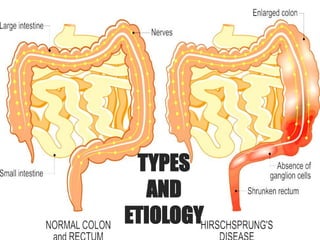
- It is a congenital disorder characterized by the absence of nerves in parts of the intestine.
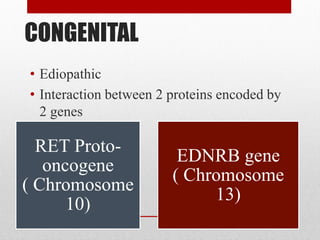
- It occurs due to improper formation of enteric nerves during embryonic development.
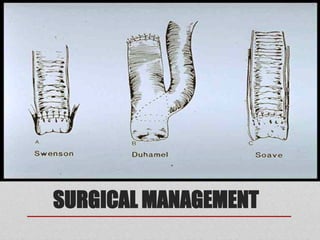
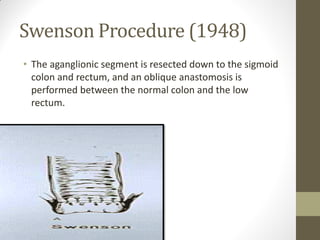
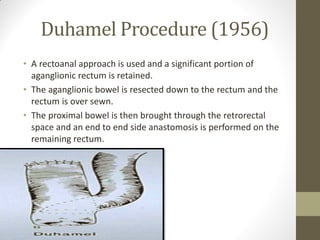
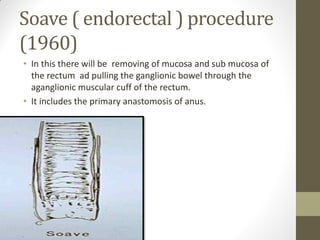
- Surgical procedures like Swenson, Duhamel, and Soave procedures are used to treat it along with medical management of complications.
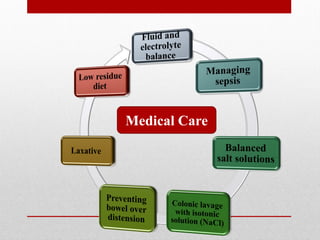
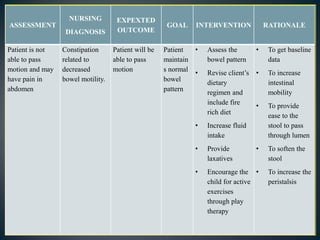
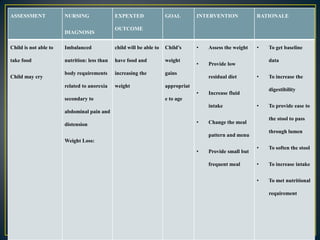
- Nursing care involves managing constipation, nutrition, pain, and caring for potential colostomies. Prognosis is generally good though some patients may have long-term bowel dysfunction.