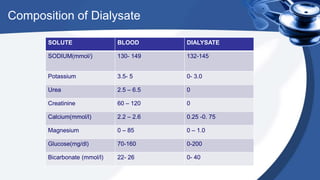
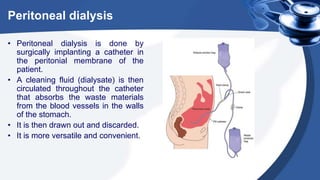
Renal replacement therapy encompasses life-supporting treatments for renal failure, including hemodialysis and peritoneal dialysis. The document details the mechanisms of these therapies, complications, vascular access methods, and nursing management before, during, and after dialysis. It also discusses indications and contraindications for each type of dialysis and the role of various medications and techniques in the process.