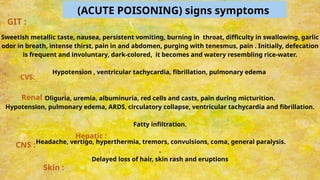
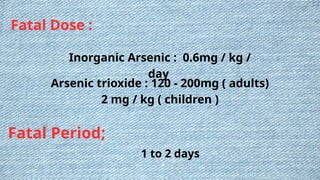
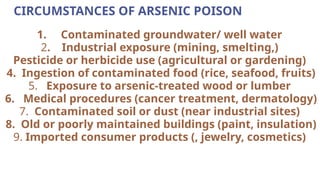
The document discusses various inorganic metallic irritants, including arsenic, mercury, lead, and copper, detailing their toxic compounds, mechanisms of action, symptoms of poisoning, and treatment protocols. Arsenic and mercury are highlighted for their acute and chronic toxicity, while lead's cumulative effects and copper's specific symptoms of poisoning, such as gastrointestinal and neurological disturbances, are also covered. Treatment for these metal poisons typically involves removal from exposure, gastric decontamination, and chelation therapy, depending on the metal involved.











































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










