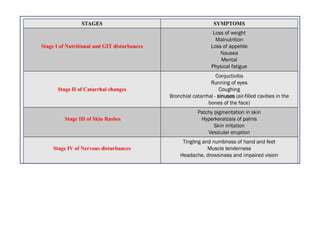
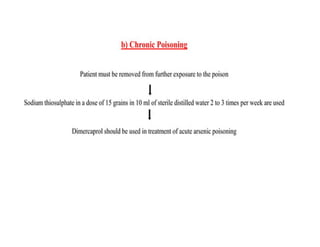
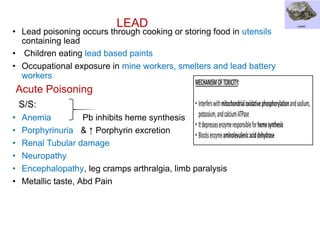
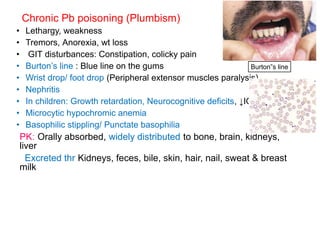
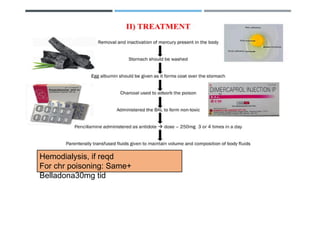
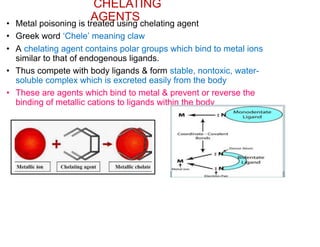
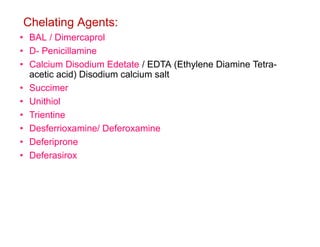
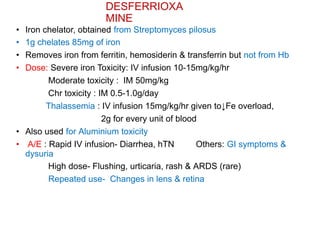
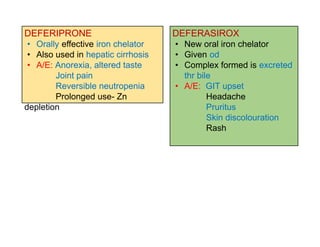
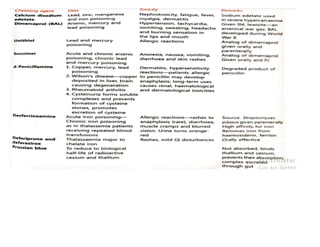
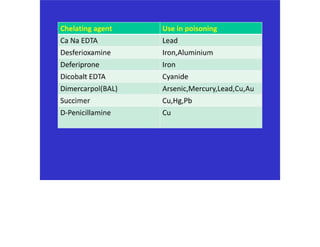
The document discusses heavy metal poisoning, highlighting the sources, symptoms, and treatment options including the use of chelating agents. It details specific heavy metals such as arsenic, lead, and mercury, their toxic effects, and the therapeutic interventions available to manage poisoning cases. The treatments include supportive care, decontamination methods, and various chelation therapies tailored to different toxic metals.