Management of Head Injuries is a document discussing the management of head injuries. It covers:
1) Head injuries are a major health hazard in India, killing over 1 million people per year from non-availability of timely treatment.
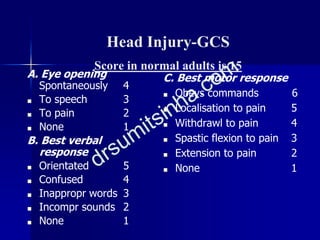
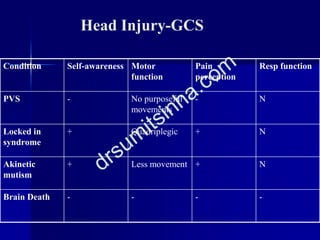
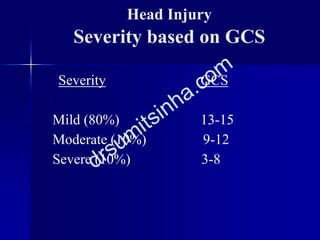
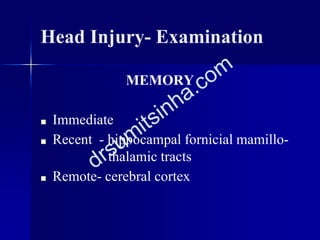
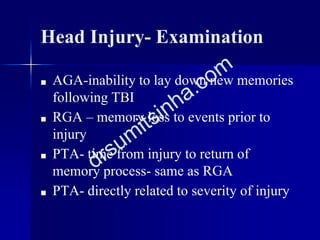
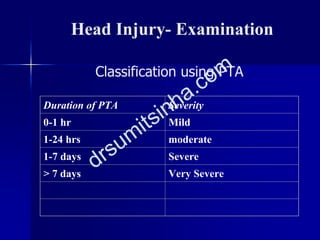
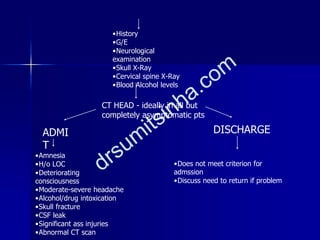
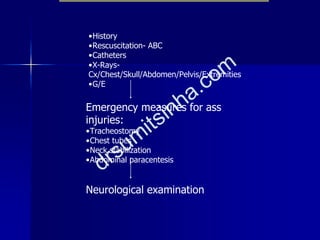
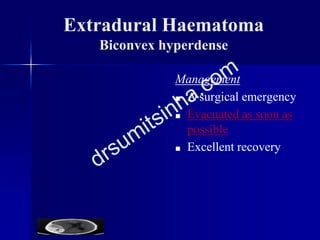
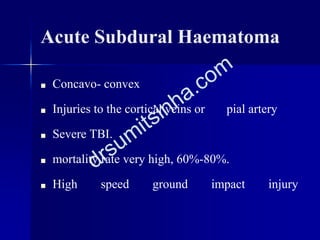
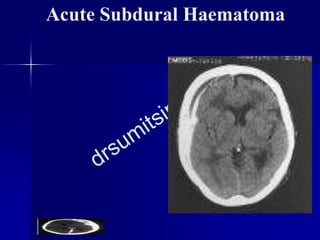
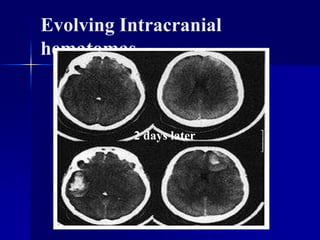
2) The document classifies head injuries and discusses examining patients including vital signs, neurological examination, Glasgow Coma Scale, and specific injuries like extradural hematomas.
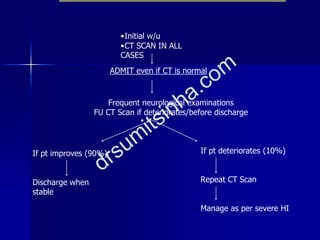
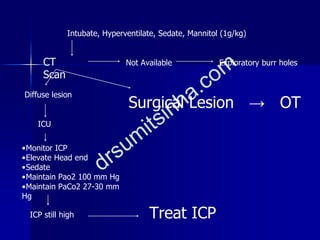
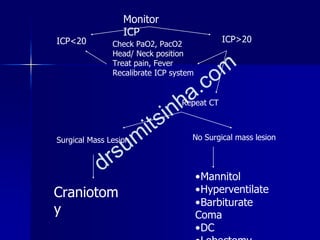
3) Initial management focuses on the ABCs - airway, breathing, and circulation. Other priorities include diagnosis using CT scan, avoiding secondary insults like hypoxia and hypotension, and indications for surgery.