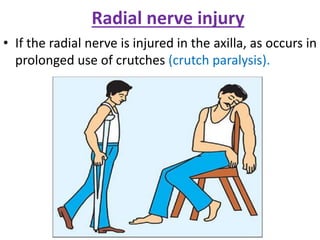
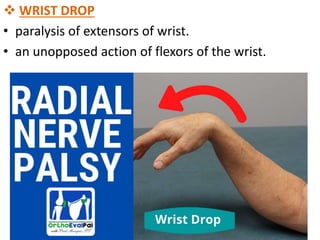
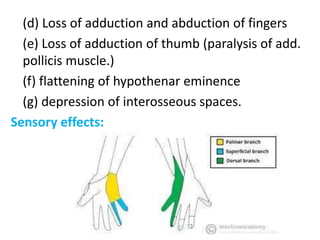
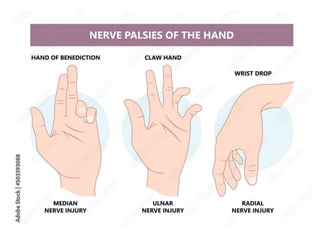
The document details clinical anatomy and common fractures of the upper limb, highlighting the clavicle as the most frequently fractured bone. It covers various fracture types such as humerus, radial, and specific conditions like 'colles' and 'smith’s' fractures, along with their symptoms and implications. Additionally, it examines dislocation mechanisms, nerve injuries, and associated clinical signs relevant to upper limb anatomy and conditions.