Downloaded 159 times

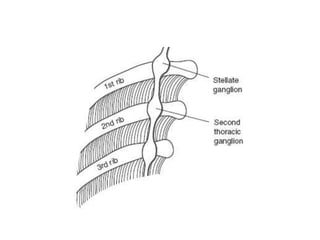

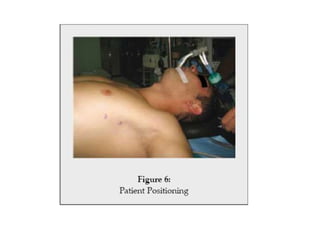
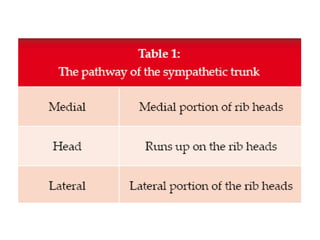


This document discusses cervical sympathectomy and thoracoscopic sympathectomy. Cervical sympathectomy involves resection of the sympathetic ganglia between the 2nd and 5th thoracic levels to treat hyperhidrosis, Raynaud's disease, and other conditions. Thoracoscopic sympathectomy is now the preferred approach and involves using video assistance and two ports to access and divide the sympathetic chain and ganglia from the 2nd to 4th thoracic levels to treat various conditions. Compensatory sweating is a common complication after sympathectomy.


















































































![Getting Started with Apache Spark: Big Data Made Simple [Free Meetup]](https://cdn.slidesharecdn.com/ss_thumbnails/apachesparkgettingstarted-260203175547-8361bcc3-thumbnail.jpg?width=640&height=640&fit=bounds)



