Downloaded 218 times








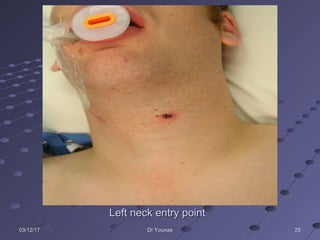





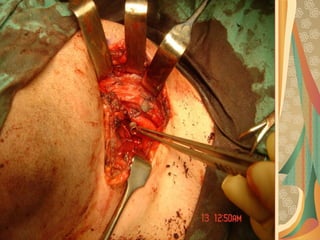

Gunshot injuries can cause complex wound patterns depending on factors like the velocity, size, and composition of the bullet. Management involves addressing airway, breathing, circulation, and hemorrhage control emergently. Evaluation with imaging helps determine the extent of injuries. Treatment follows a phase approach, starting with wound toilet, debridement, and stabilization before later reconstruction with bone grafts and soft tissue flaps to restore function and appearance. Special considerations include injuries to structures like the facial nerve and salivary ducts. Penetrating neck injuries from gunshots also carry risk of damaging vital vasculature.











































































































