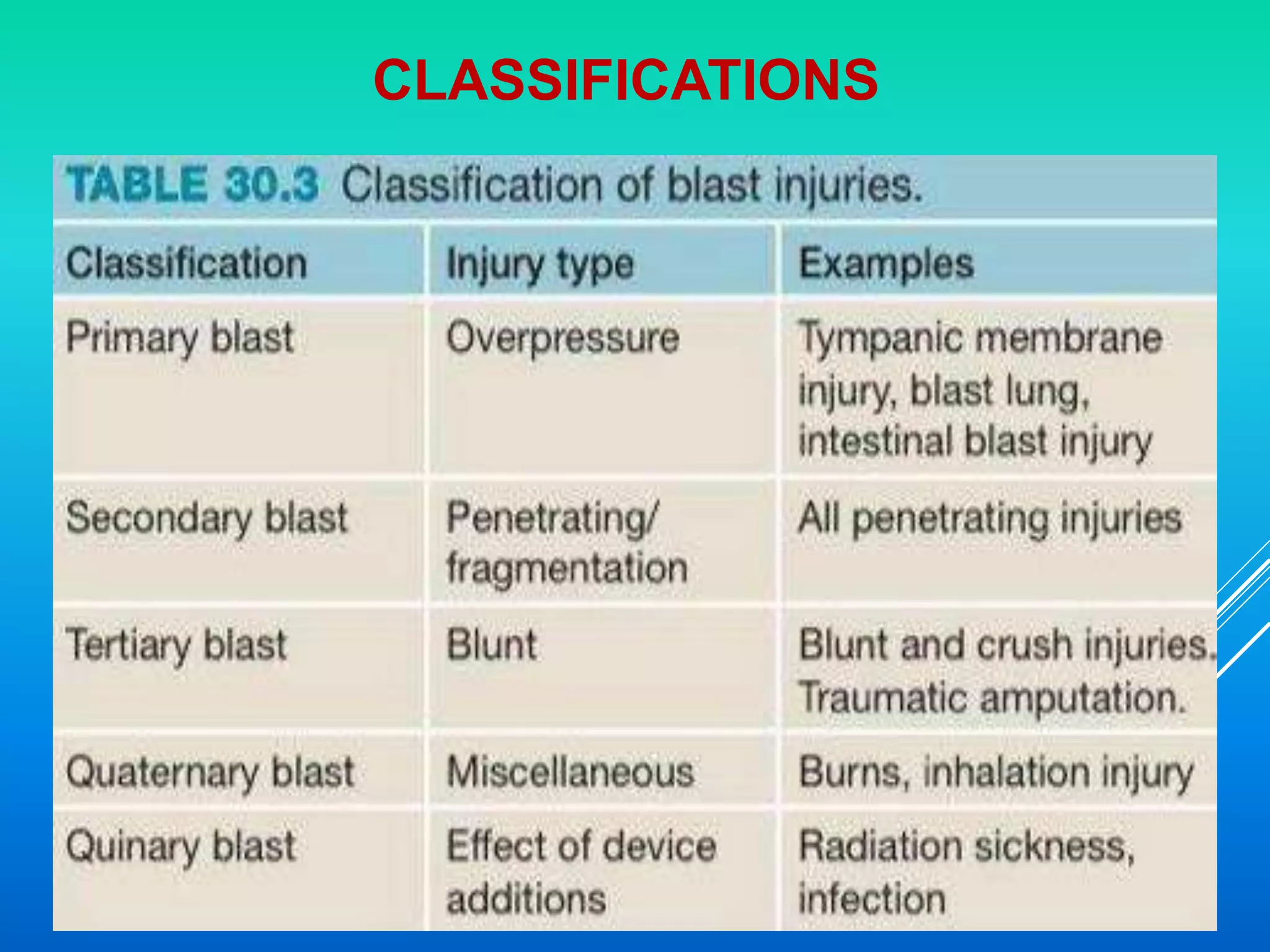
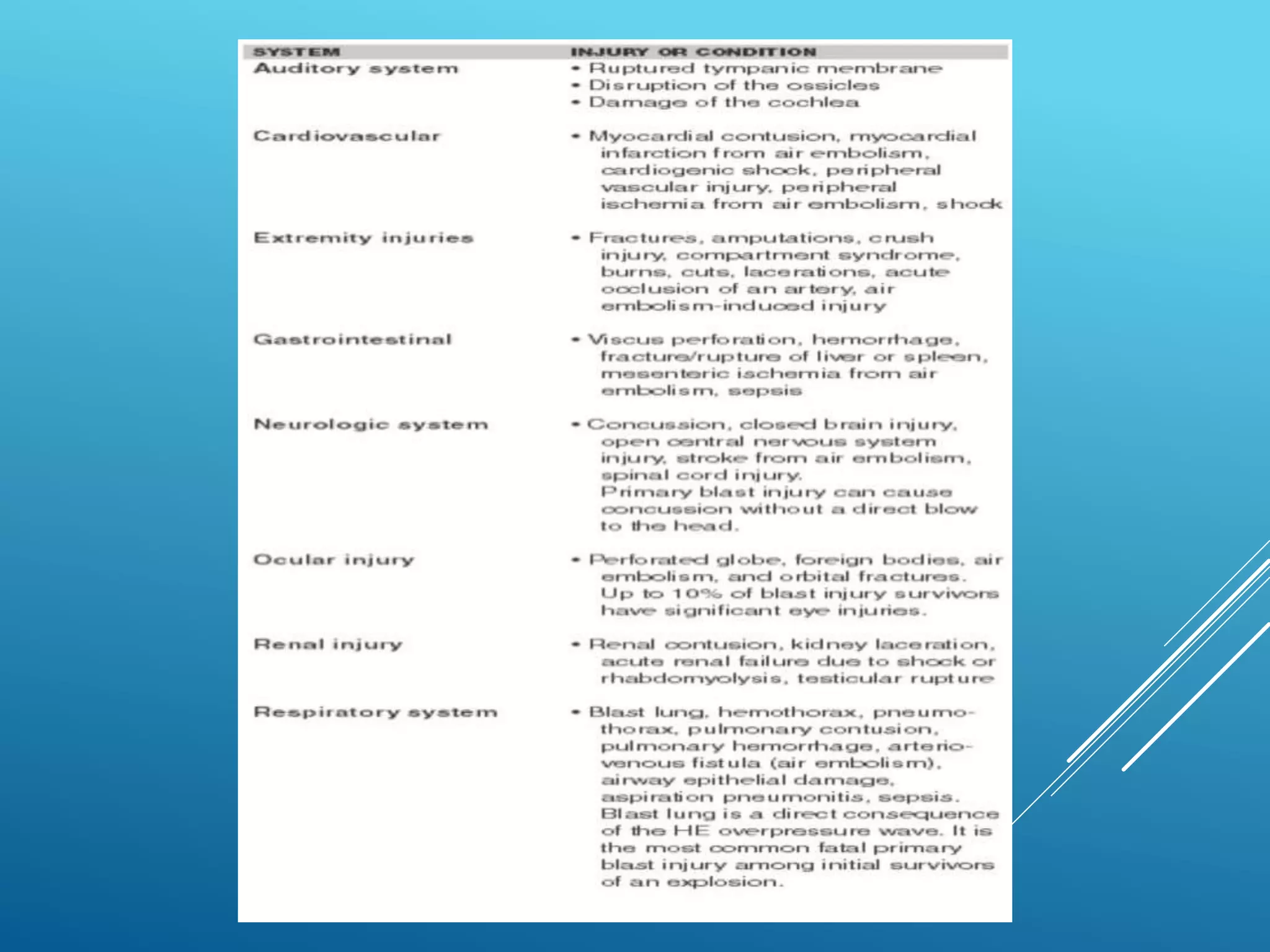
This document discusses blast and missile injuries. It defines a blast injury as physical trauma resulting from an explosion. Blast injuries can include internal organ damage, extremity injuries, burns, and injuries to hearing and vision. The mechanisms of injury are classified as primary (direct blast wave), secondary (fragmentation), tertiary (displacement), or quaternary (burns, toxins). Factors like the explosive type, victim characteristics, and environment impact injuries. Common injuries include abdominal wounds, vascular and neurological trauma. Treatment priorities are ABCs, antibiotics, tetanus prophylaxis, debridement, wound care, fasciotomies, stabilization, and definitive care based on injuries.