Downloaded 297 times
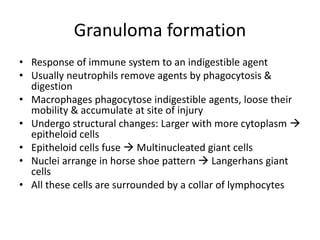
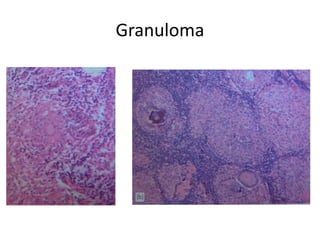
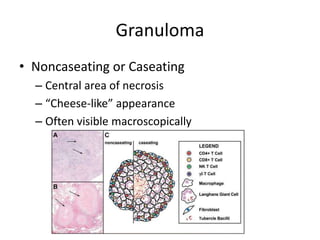
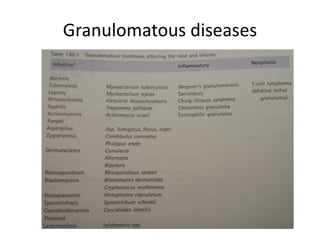

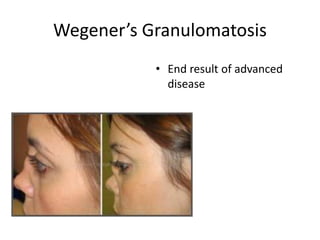
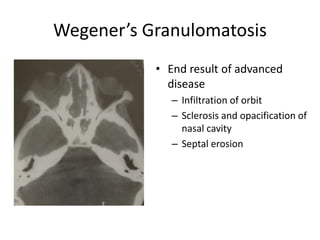
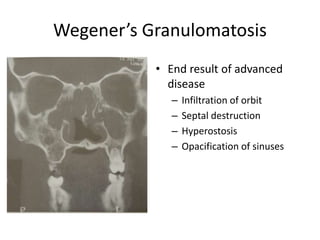
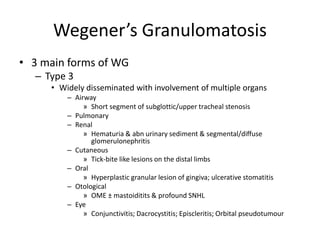
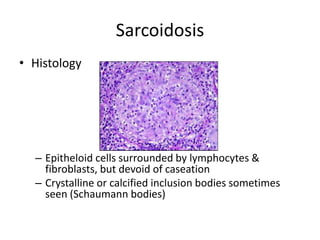
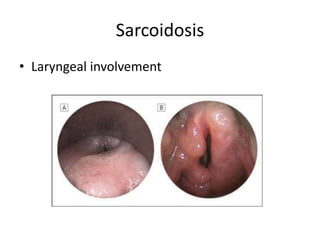
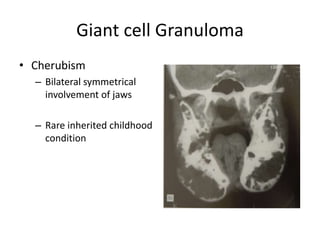
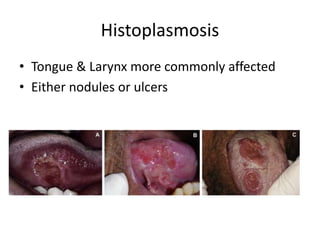
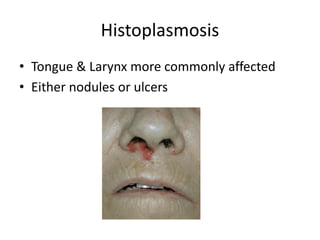

The document discusses various granulomatous diseases affecting the upper respiratory tract, including Wegener's granulomatosis, sarcoidosis, Churg-Strauss syndrome, and other infectious systemic diseases such as tuberculosis and leprosy. It provides detailed information on the etiology, clinical features, histology, diagnosis, and treatment options for these conditions. The significance of granuloma formation as a response of the immune system to indigestible agents is emphasized throughout the document.




















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














