1) The document discusses different types of abscesses that can occur in the pharynx and neck region, including peritonsillar abscesses, parapharyngeal abscesses, and submandibular space abscesses (Ludwig's angina).
2) It describes the anatomy, etiology, clinical features, investigations, treatment, and complications of each type of abscess. Recurrent tonsillitis and dental infections are common causes.
3) Symptoms include pain, difficulty swallowing, trismus, and in severe cases, airway obstruction. Treatment involves antibiotics, analgesics, and sometimes surgical drainage or tracheostomy.
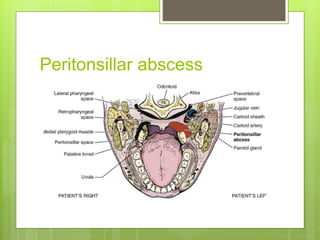
![Peritonsillar Abscess [Quinsy]
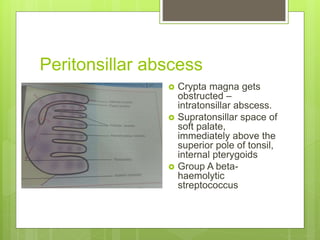
Definition – acute inflammation of the
peritonsillar space.
Place – lies between superior constrictor
muscle & the tonsillar capsule.
Etiology – Recurrent attacks of tonsillitis
- Trauma or Foreign body
- Dental infections & surrounding areas
- Immunocompromised status](https://image.slidesharecdn.com/abscessesofpharynx-160404162943/85/Abscesses-of-pharynx-2-320.jpg)
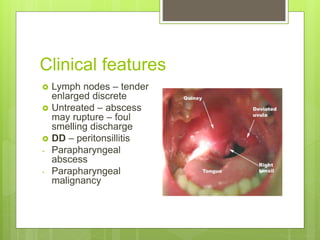
![Clinical features
Symptoms –
General – fever, chills & rigor, malaise, body
aches & toxic features
Local –odynophagia [ severe ]
Otalgia
Neck pain
Trismus – pterygoid muscle spasm
Muffled speech – hot potato voice](https://image.slidesharecdn.com/abscessesofpharynx-160404162943/85/Abscesses-of-pharynx-5-320.jpg)
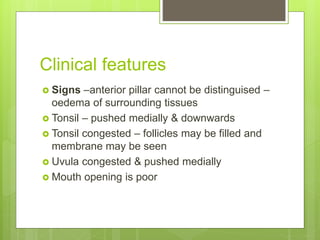


![Clinical features
Etiology - Dental infections, tonsillitis,
sialadenitis, lymph node suppuration
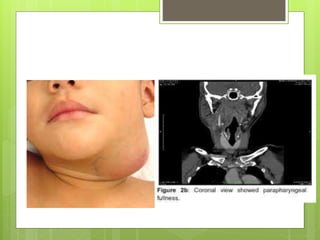
Firm induration [ swelling ], erythema – seen
lateral and anterior to sterocleidomastoid
muscle
Difficulty in flexing & turning neck
Trismus – pterygoid muscle
Dysphagia & dyspnea
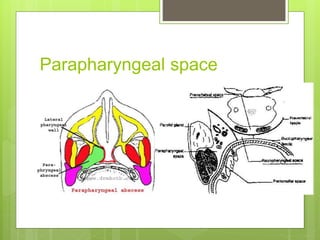
Bulge – lateral wall of pharynx](https://image.slidesharecdn.com/abscessesofpharynx-160404162943/85/Abscesses-of-pharynx-17-320.jpg)


![Complications
1] IJV – thrombosis
Shaking chills, spiking fever, prostration
Tenderness at angle of mandible & along SCM
muscle
Asso. Bacteremia, pulmonary emboli, suppurative
subclavian phlebitis, lateral sinus thrombosis,
brain abscess, metastatic abscess
Treatment – prolonged antibiotics, surgical
drainage, ligation of involved vein.](https://image.slidesharecdn.com/abscessesofpharynx-160404162943/85/Abscesses-of-pharynx-22-320.jpg)
![Complications
2] Carotid artery rupture
- false aneurysm formation
- herald bleeds – before major bleed
- ICA – common involvement
3] Laryngeal edema
4] Mediastinitis](https://image.slidesharecdn.com/abscessesofpharynx-160404162943/85/Abscesses-of-pharynx-23-320.jpg)
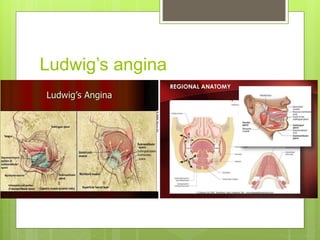
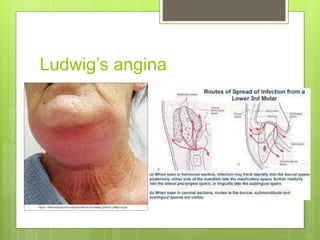
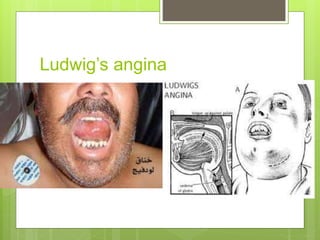
![Submandibular space abscess [
LUDWIG’S ANGINA ]
Inflammation of the submaxillary and
sublingual space
Cellulitis without lymphatic involvement –
causing massive swelling of tongue & floor of
mouth.
Fatal – respiratory obstruction](https://image.slidesharecdn.com/abscessesofpharynx-160404162943/85/Abscesses-of-pharynx-24-320.jpg)