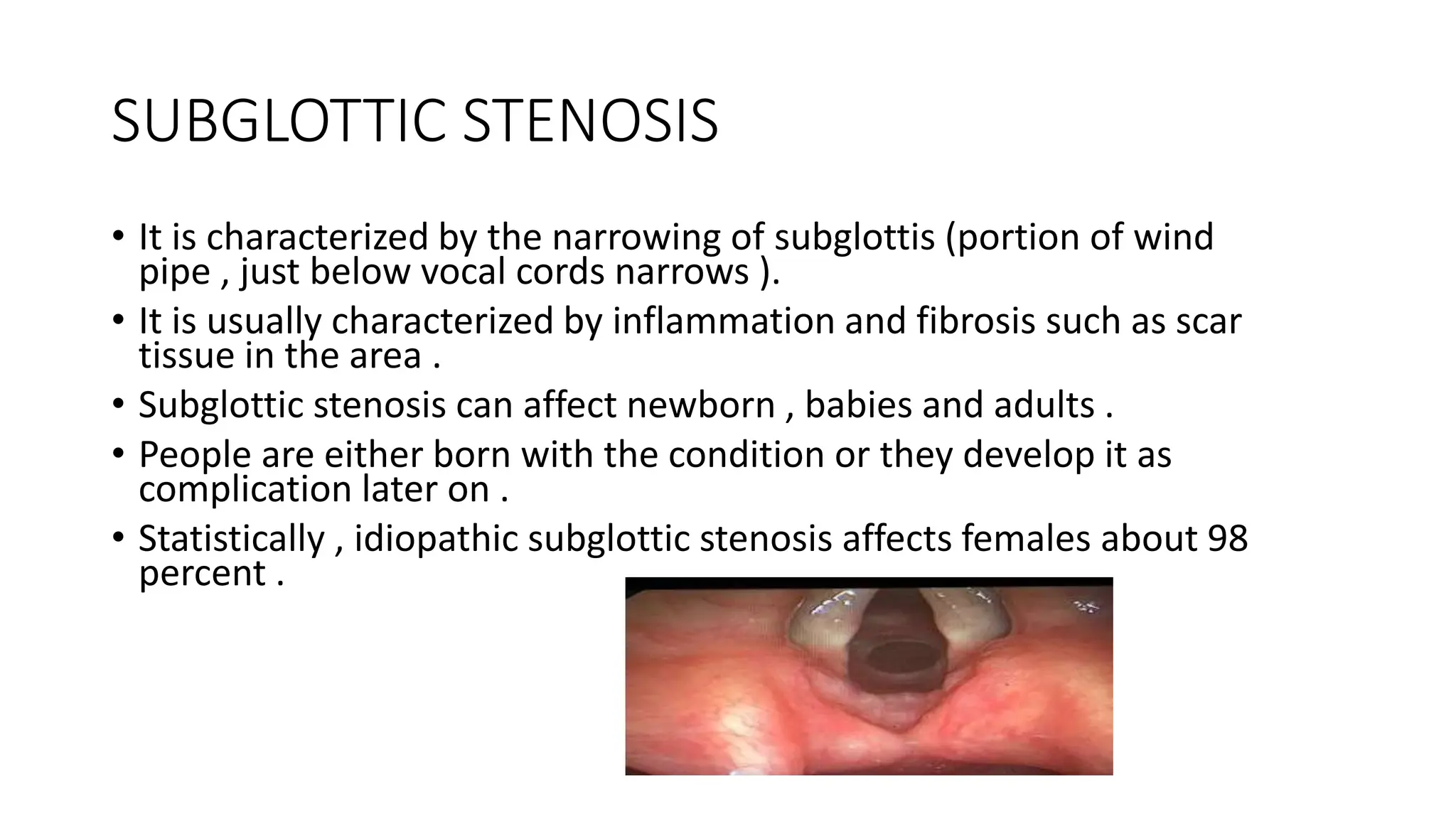
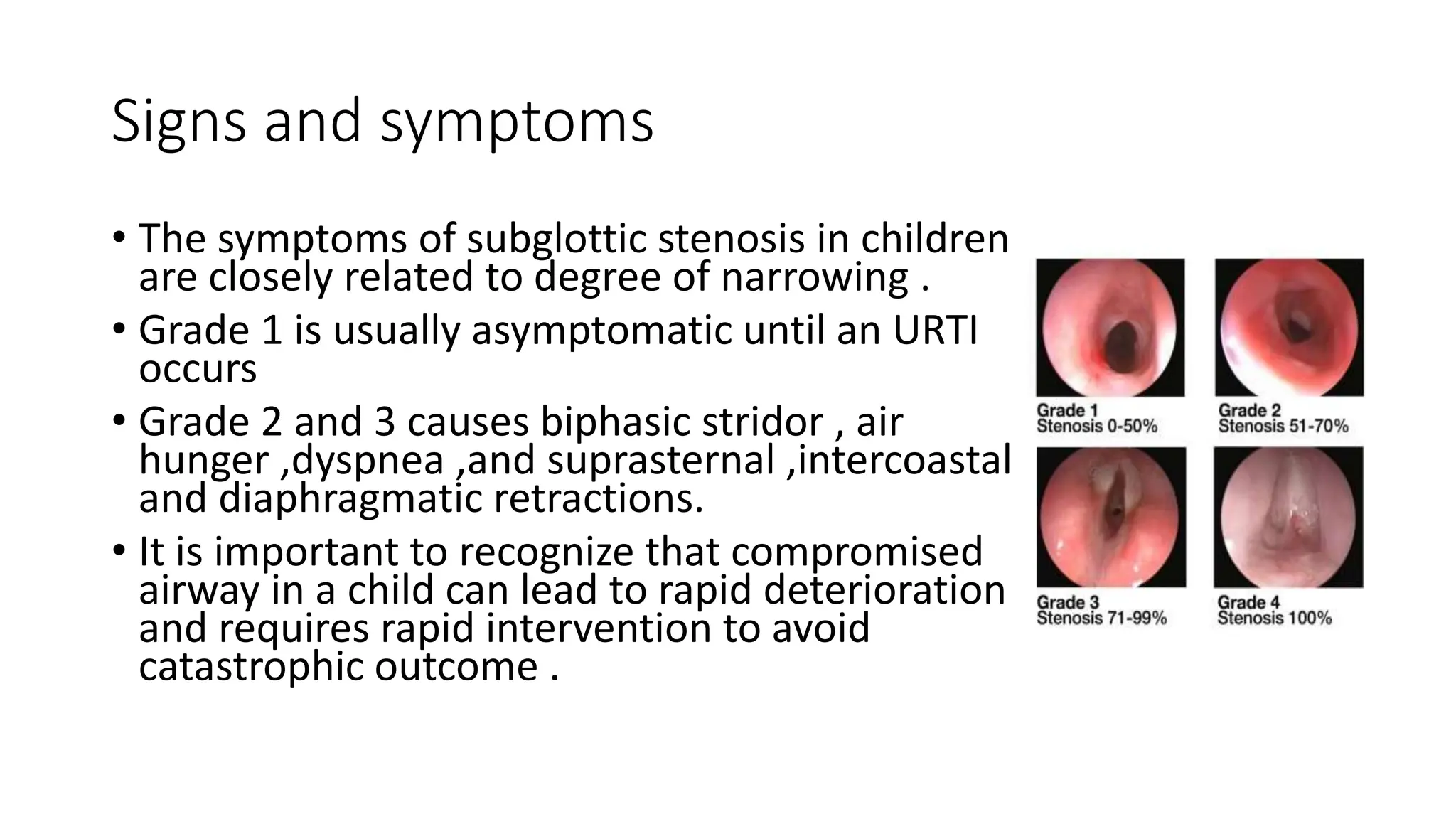
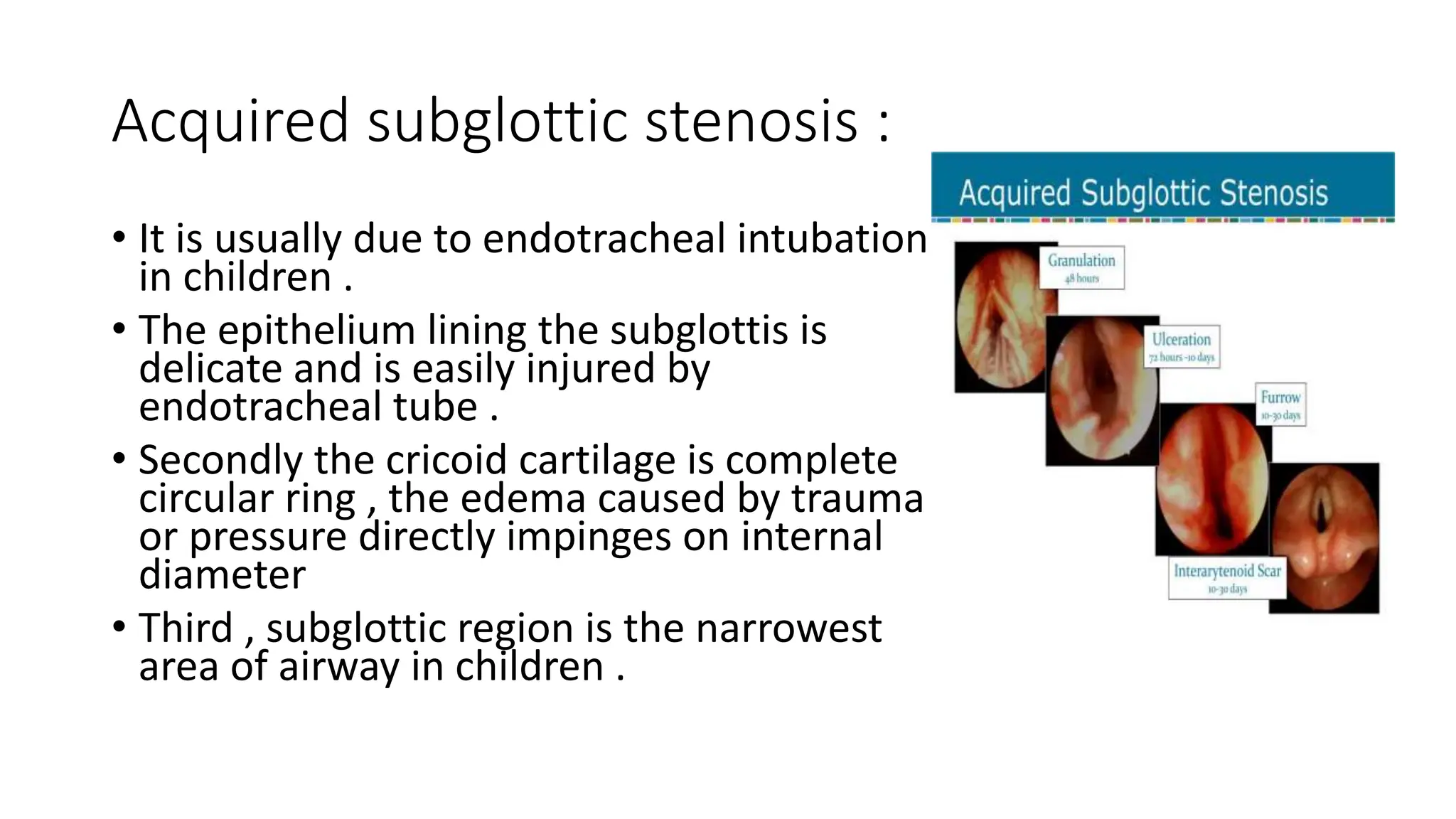
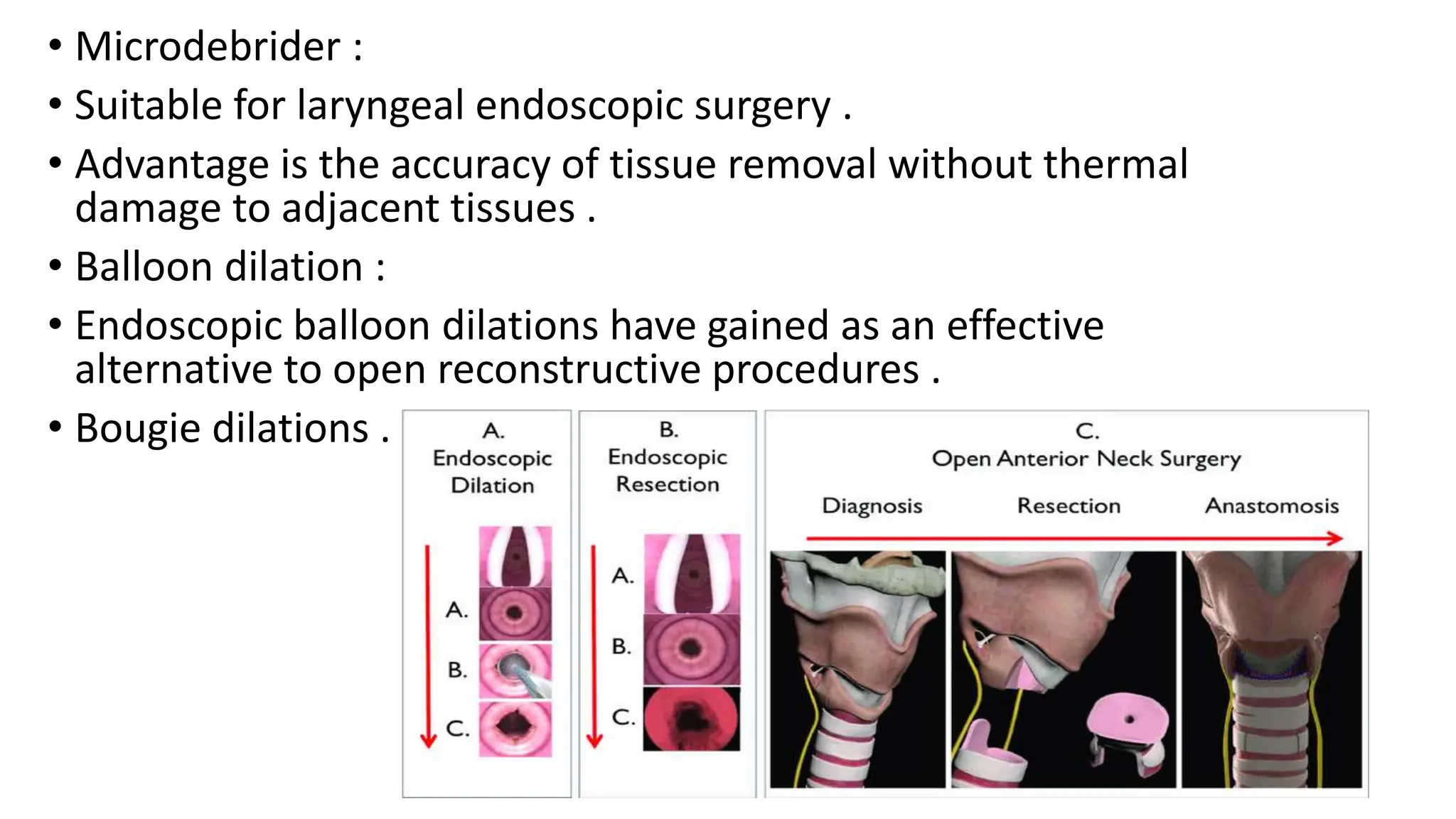
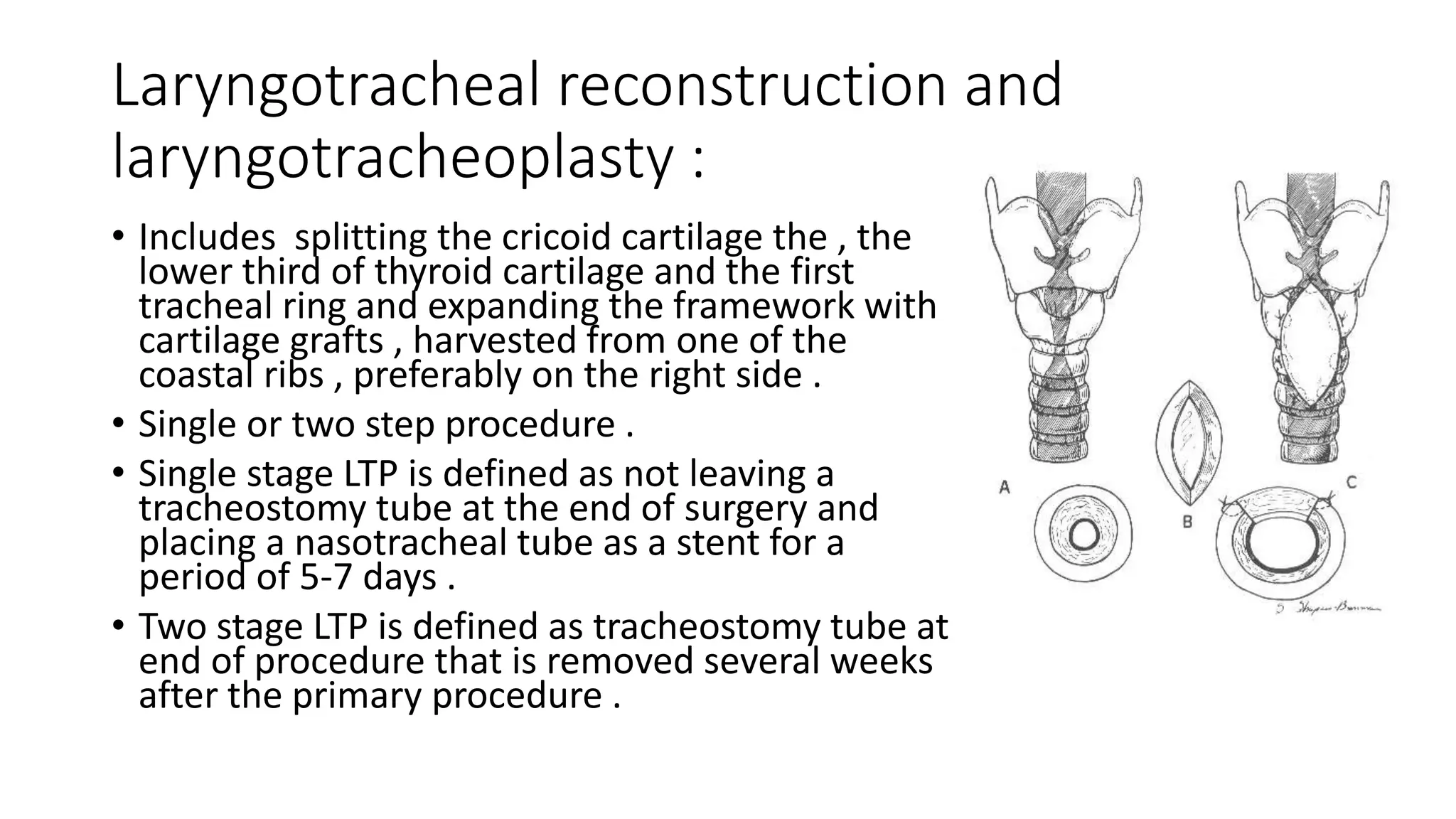
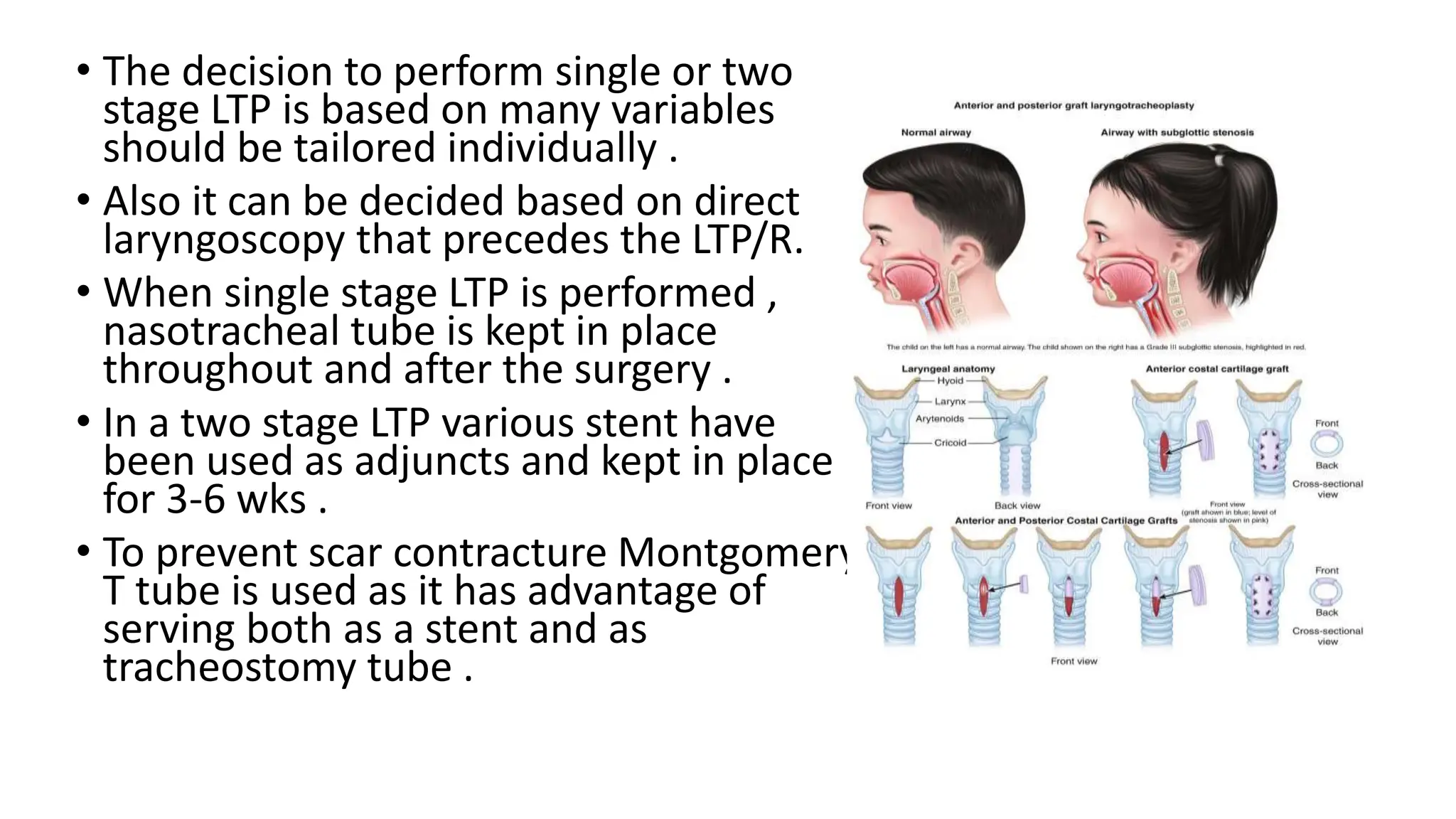
This document summarizes subglottic stenosis, which is a narrowing of the windpipe just below the vocal cords. It can be congenital, meaning present at birth, or acquired later due to trauma, infection, or intubation. Symptoms include shortness of breath, stridor, and cough. It is graded based on the percentage of obstruction. Treatment depends on the grade but may include observation, endoscopic procedures like dilation or laser treatment, stents, or open procedures like tracheostomy, laryngotracheal reconstruction, or partial cricotracheal resection. The goal is to restore an open airway while minimizing scarring.