
Download to read offline
![RFs:
Hypertension the most common comorbidity (58%).
DM(24%)
Cardiovascular disease (23.8%)
Nephropathy (15%)
AF (14.3%) [13,54], particularly in IRCI cases.
A history of previous surgery (i.e.GI surgery, abdominal aortic aneurysm
surgery, or major CV surgery) in 3.9—79.1%
Predictors of a poor prognosis are male gender, tachycardia, absence of
rectal bleeding, peritonitis, shock, hypotension (<90 mmHg) &IRCI.](https://image.slidesharecdn.com/gitjclubcolonischemia22-220128132446/85/Git-j-club-colon-ischemia22-5-320.jpg)


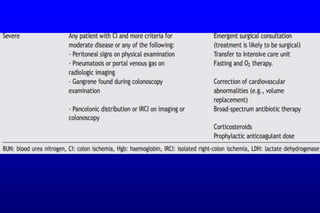
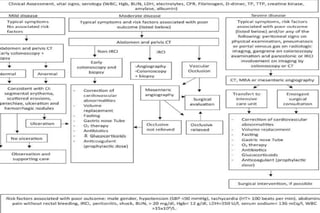
This document summarizes information about ischemic colitis (CI). CI is often underdiagnosed but is a common condition that presents with non-specific symptoms. It most frequently affects the elderly and women. Treatment depends on the severity, location and duration of the CI. Potential risk factors include hypertension, diabetes, cardiovascular disease and previous abdominal surgeries. Correct diagnosis and identification of underlying causes is important for prognosis. Surveillance endoscopies may be considered for detecting strictures. Prompt treatment is important as delays can increase mortality rates.








































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














