
Download to read offline
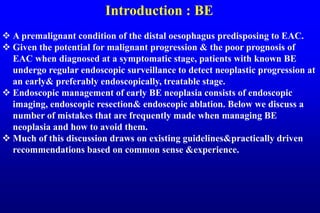
![1:Clean&inspect well
With inadequate cleaning& immediately ‘jumping’ to obtain the inevitable
random biopsy samples you will not detect the more subtle Barrett lesions.
Use the waterjet of to clean the Barrett segment;takes 1–2 minutes.
Switch to optical chromoscopy: if the oesophagus looks impeccably clean
on narrow-band imaging (NBI), then cleaning is optimal.
Spend 3–5 minutes inspecting the segment using white light endoscopy.
Switching back-forth with optical chromoscopy, help to see more.
Retroflex the endoscope to inspect the ‘danger zone’—the area where the
Barrett segment transits into the hiatal hernia,area has the highest risk of
neoplasia &highest risk of neoplasia being missed endoscopically.
Look longer, biopsy less! After taking first biopsy sample most of imaging
opportunities are lost.
Detecting early neoplasia is all about recognizing how early
neoplasia actually looks.
Excellent training modules are available at [www.best-academia.eu].](https://image.slidesharecdn.com/gitjclubbemanagementadvices22-220128133827/85/Git-j-club-be-management-advices22-3-320.jpg)
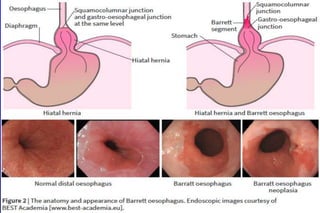
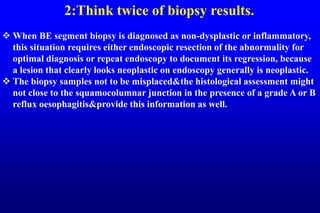
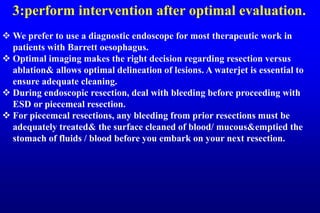
This document discusses best practices for managing Barrett's esophagus and early stage neoplasia. It provides 10 tips to avoid common mistakes in diagnosis and treatment, including thoroughly cleaning and inspecting the esophagus, considering biopsy results carefully, performing interventions only after optimal evaluation, resecting visible lesions before ablation, not ablating inflamed or swollen tissue, using marking before resection, choosing the appropriate resection technique, being properly trained, preparing for bleeding complications, and managing perforations carefully.











































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











