
Download to read offline
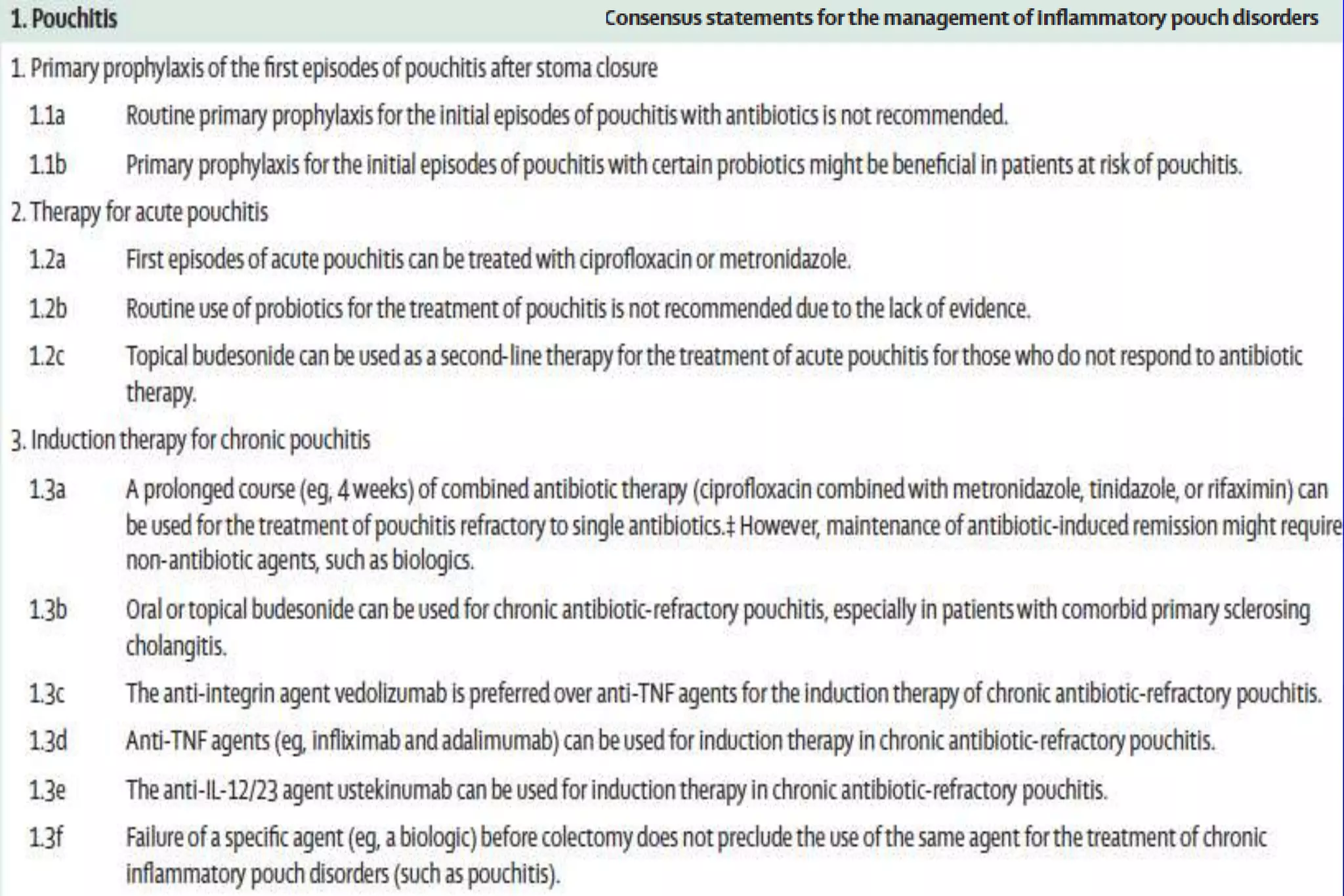
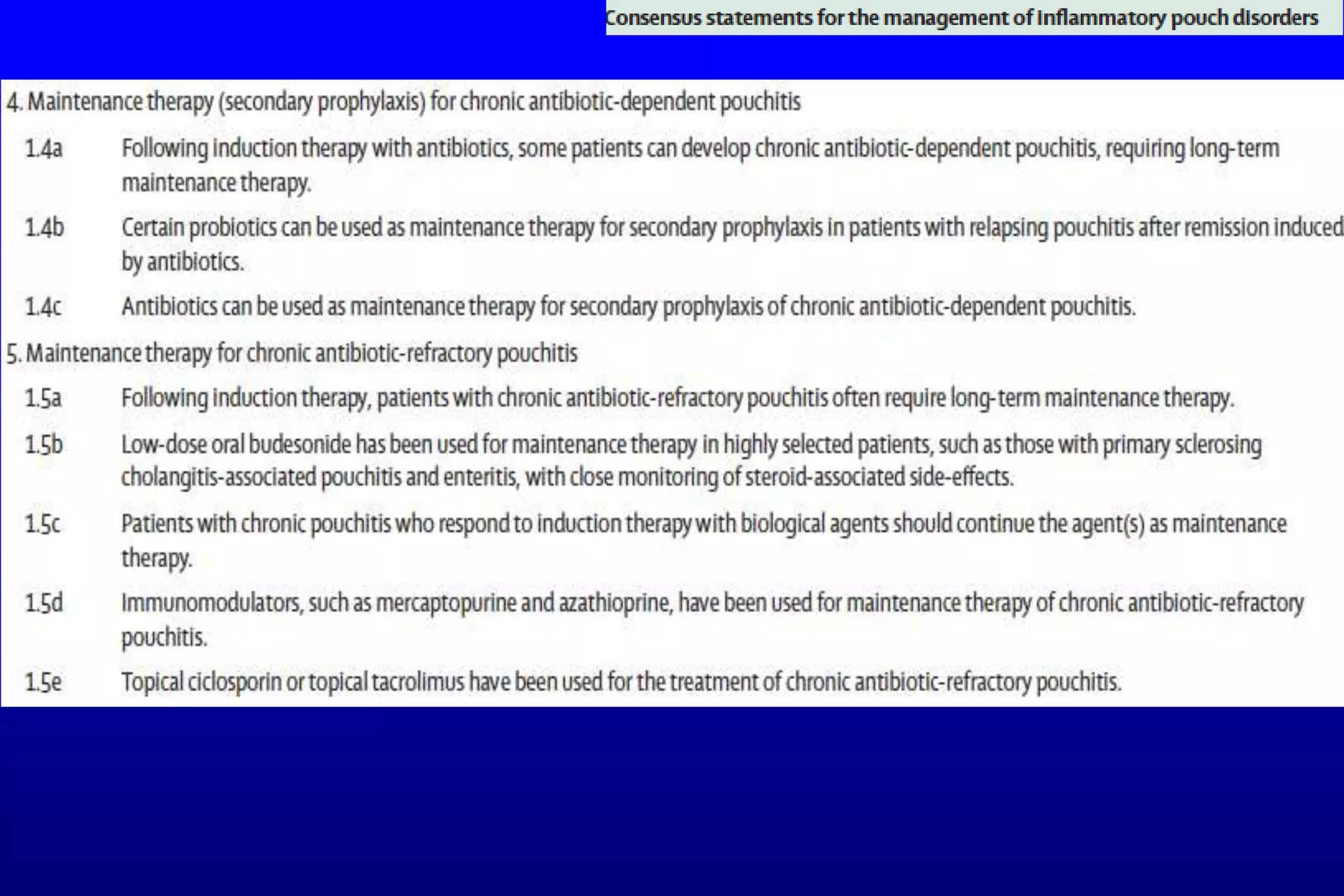
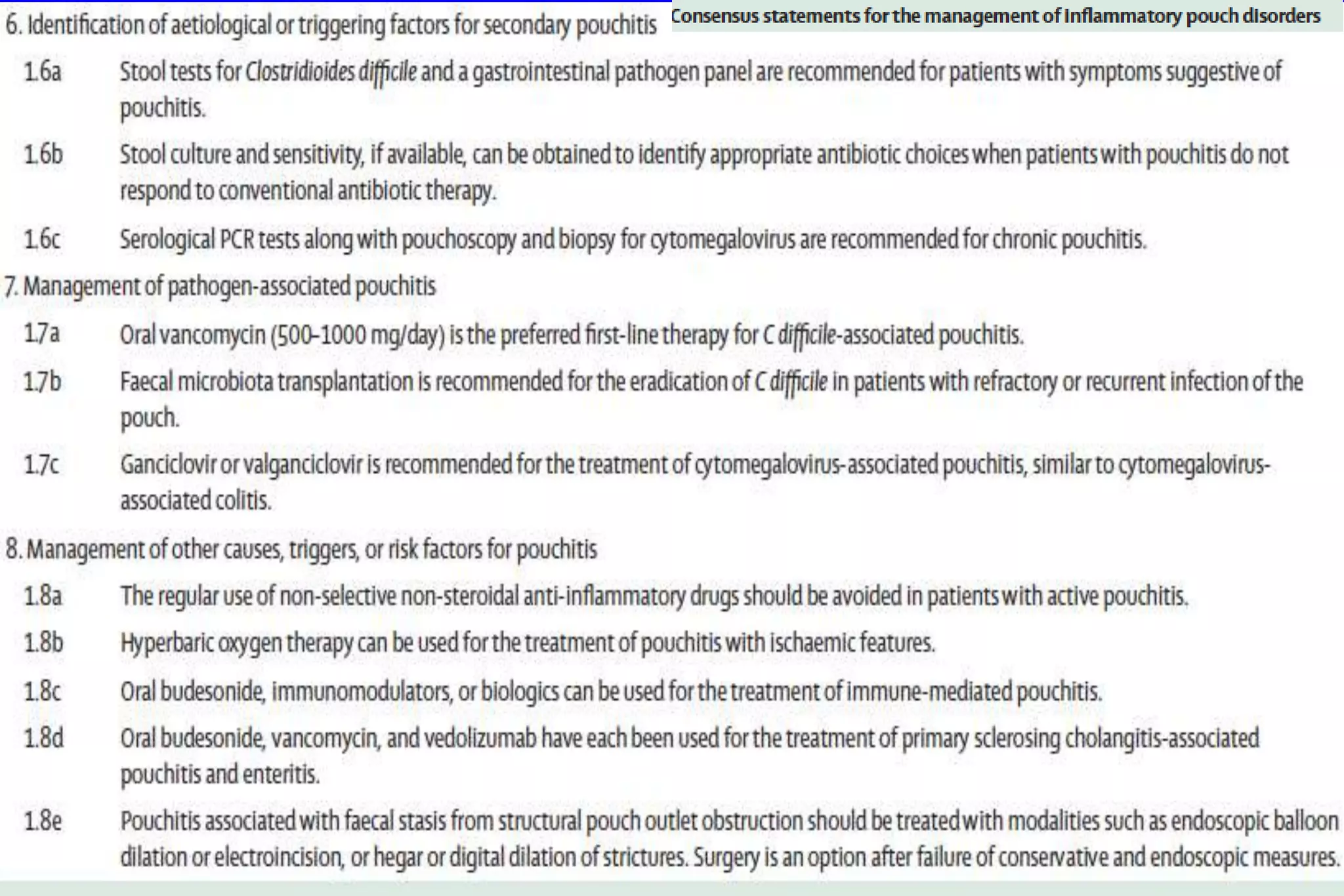
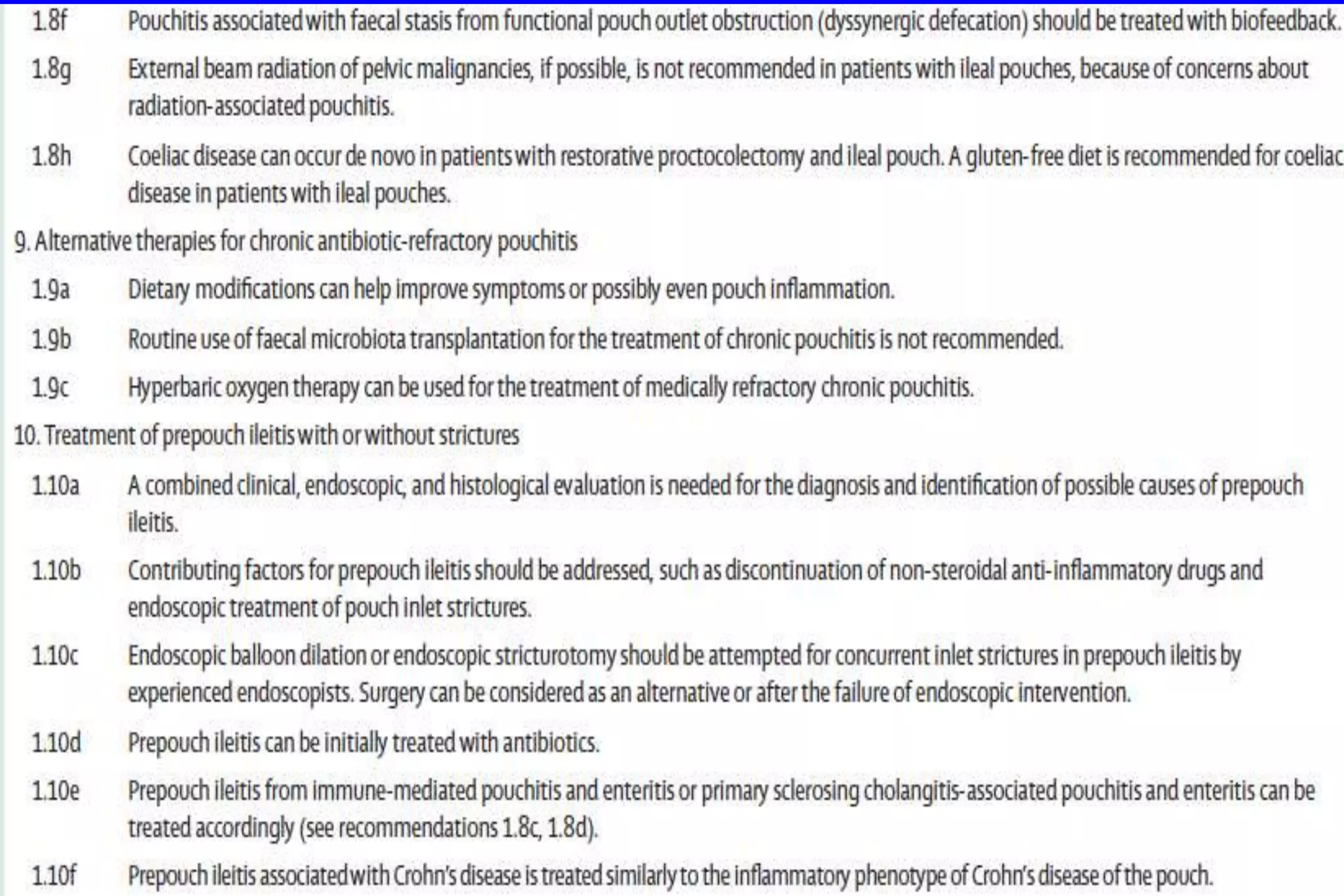
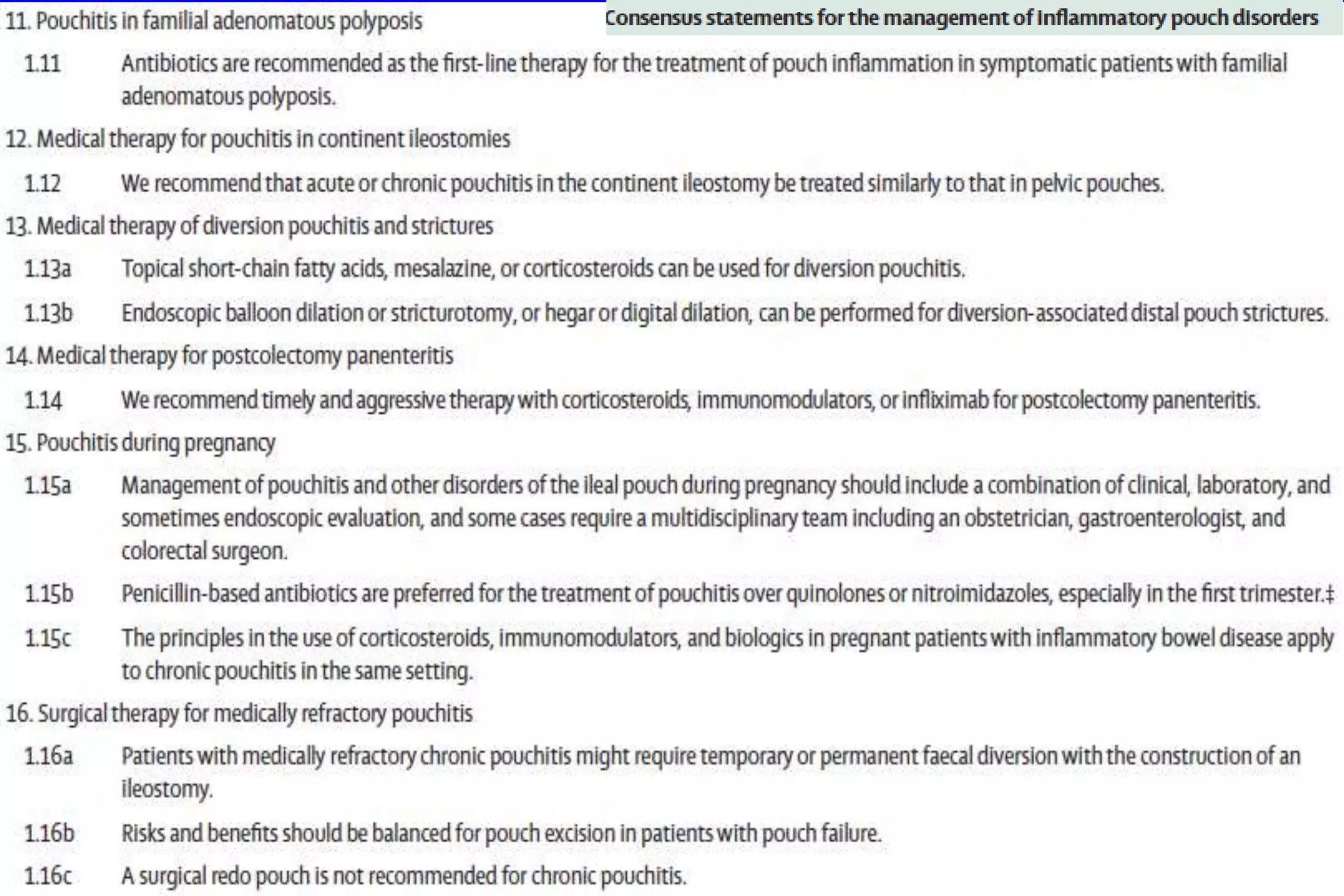
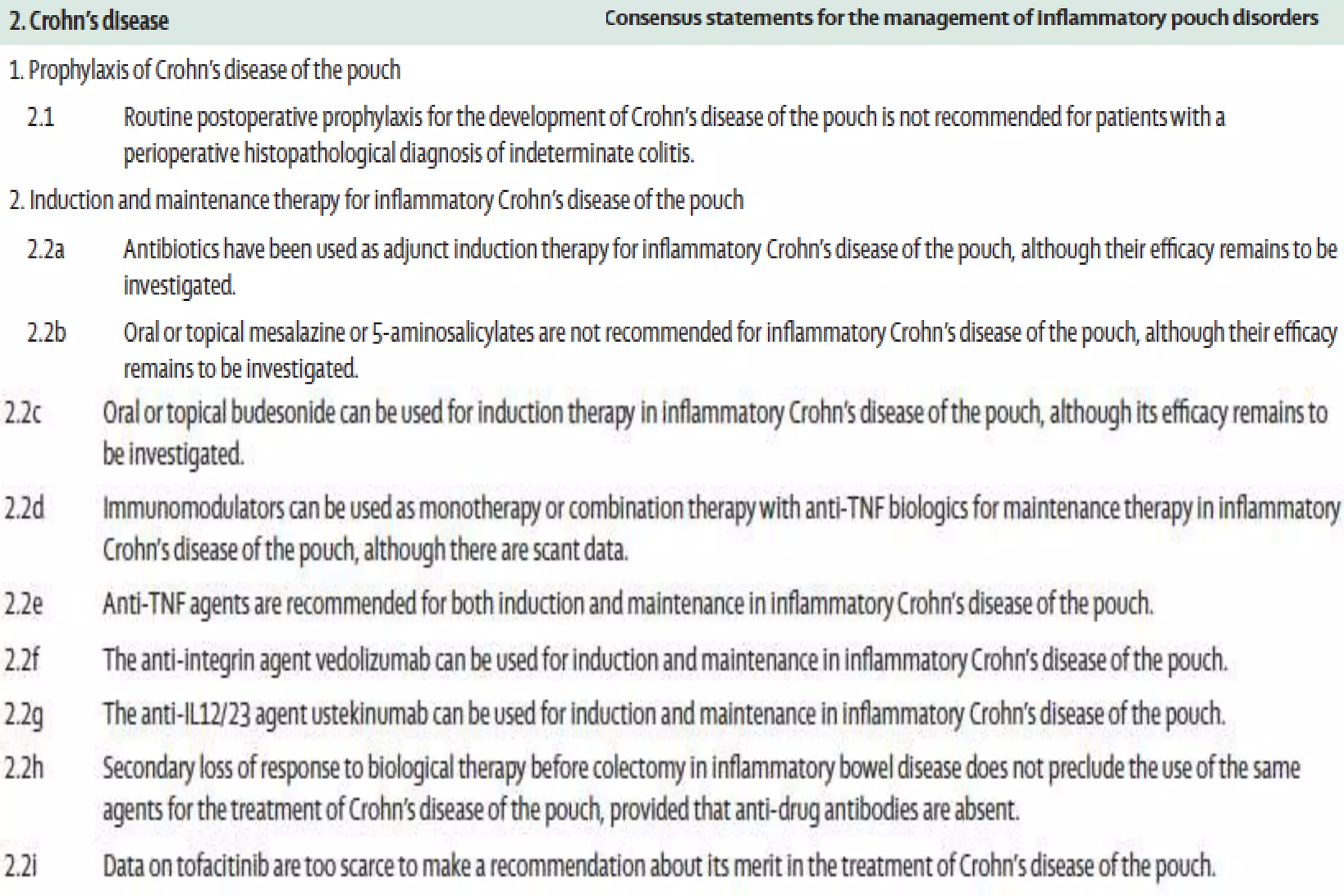
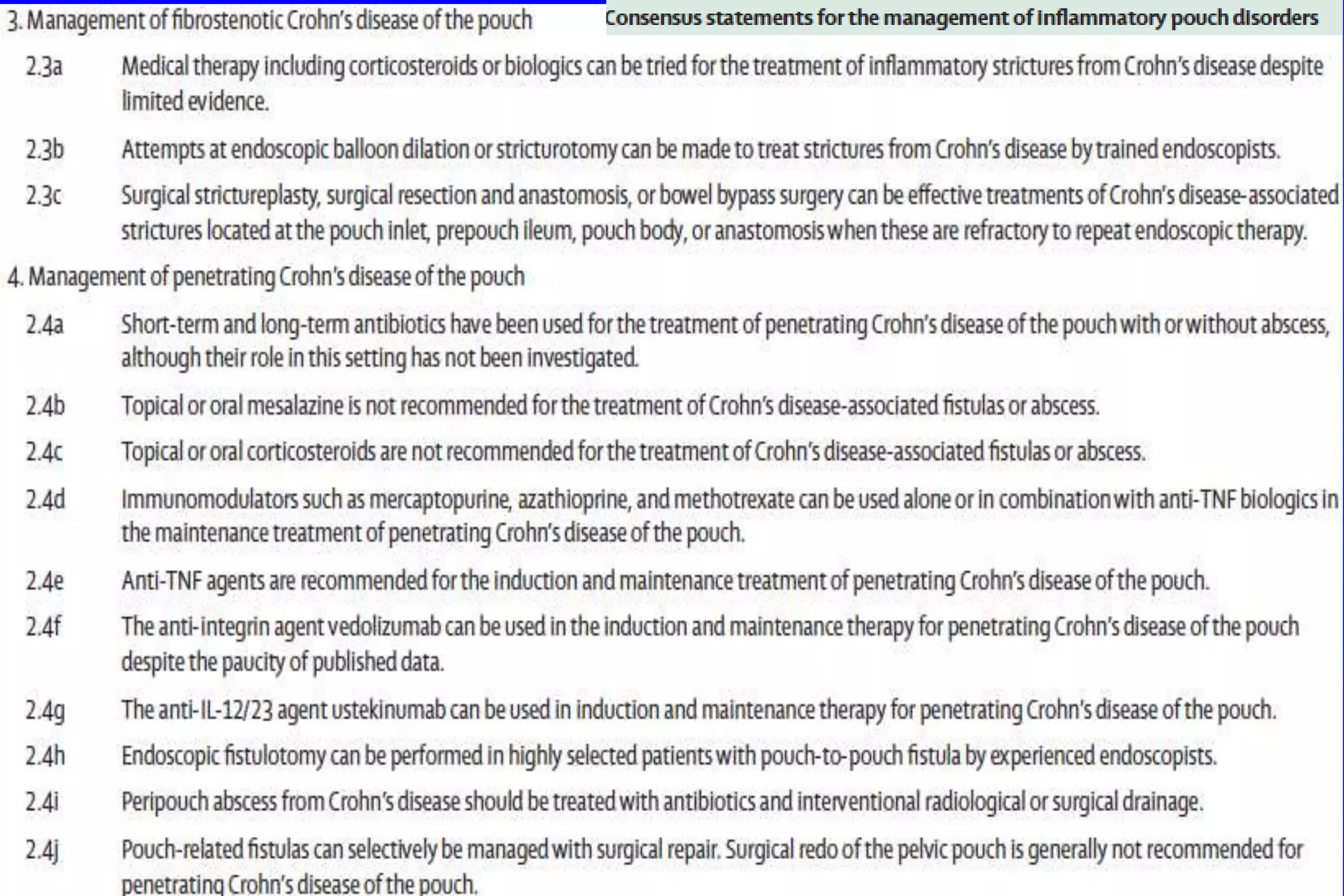
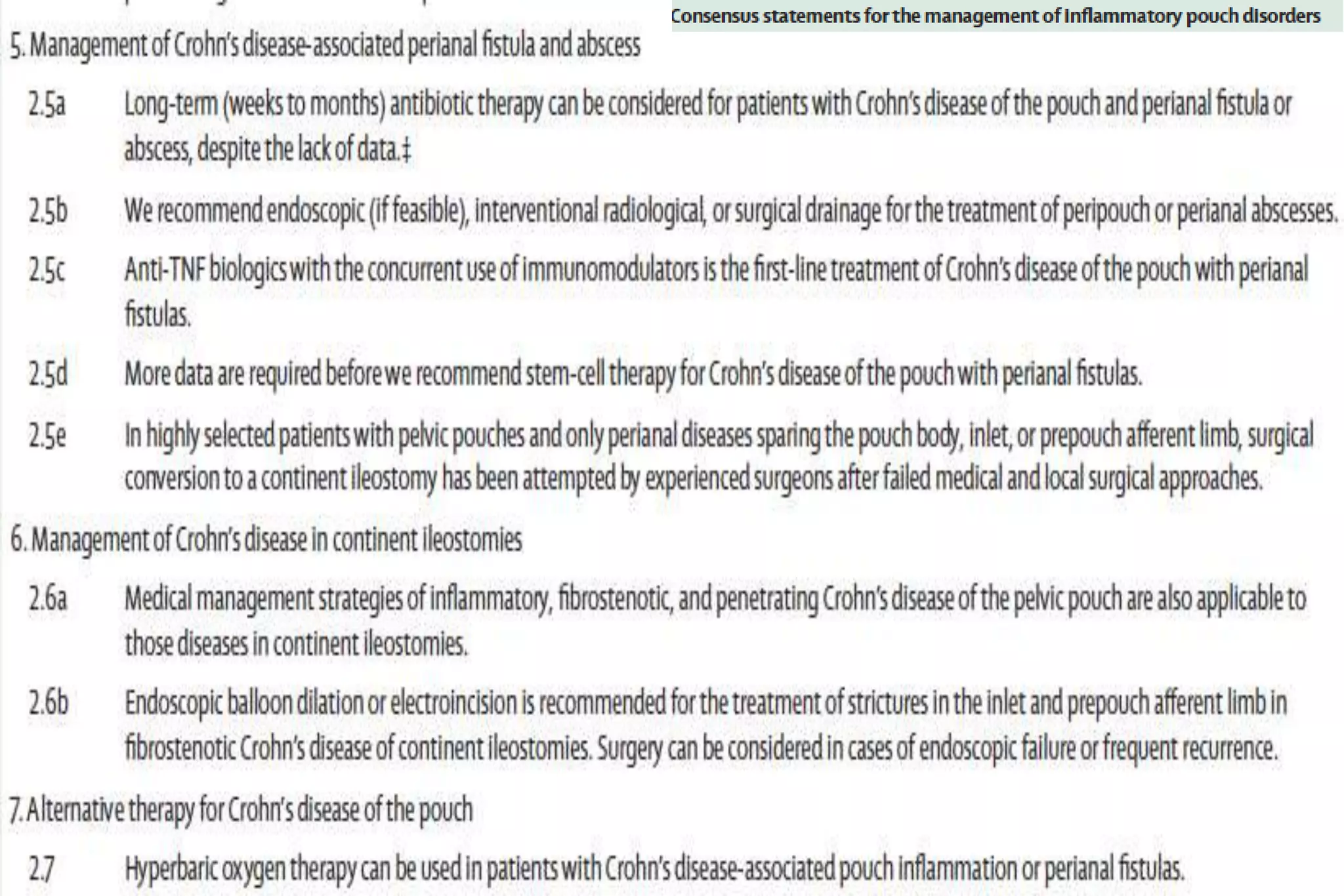
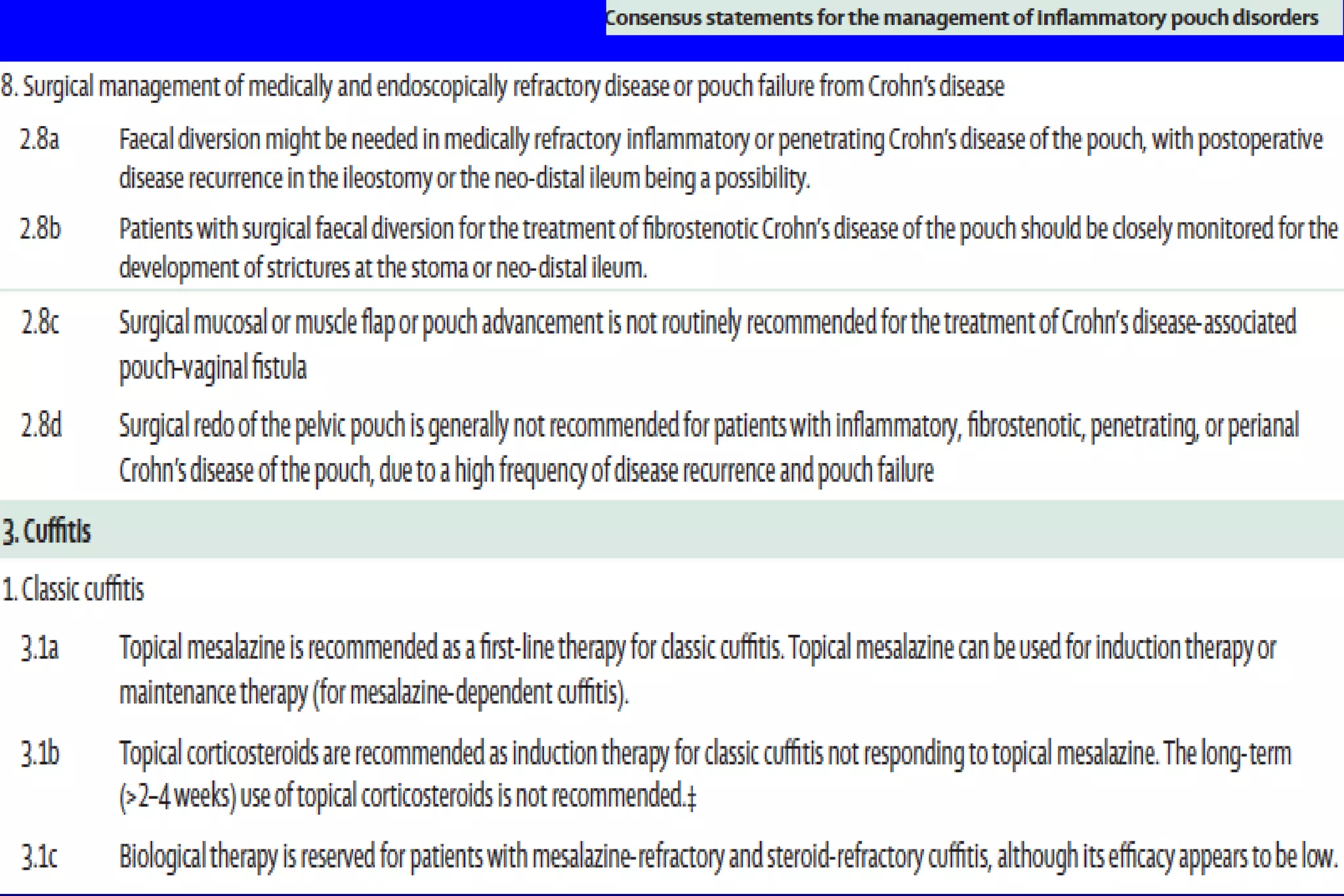
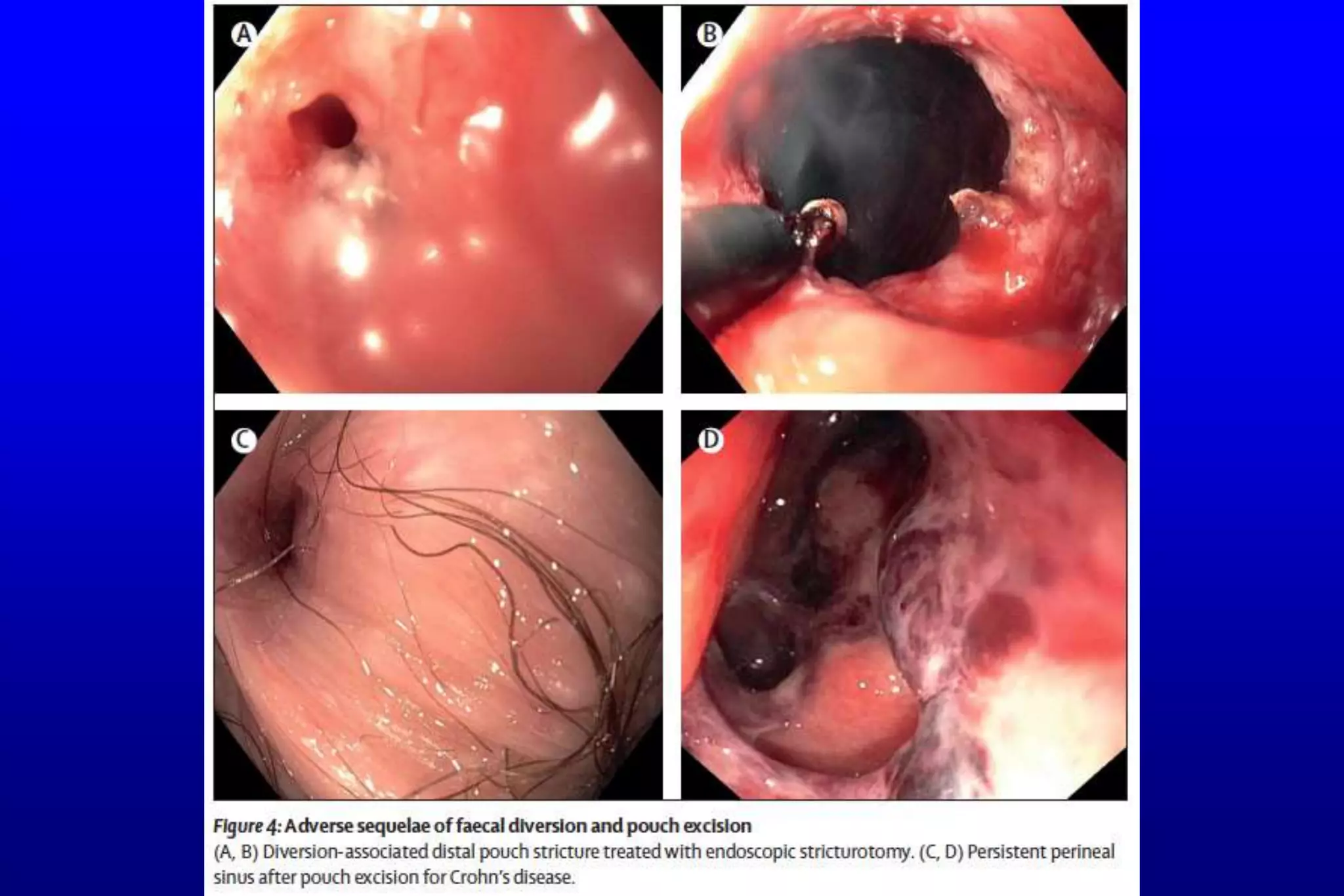
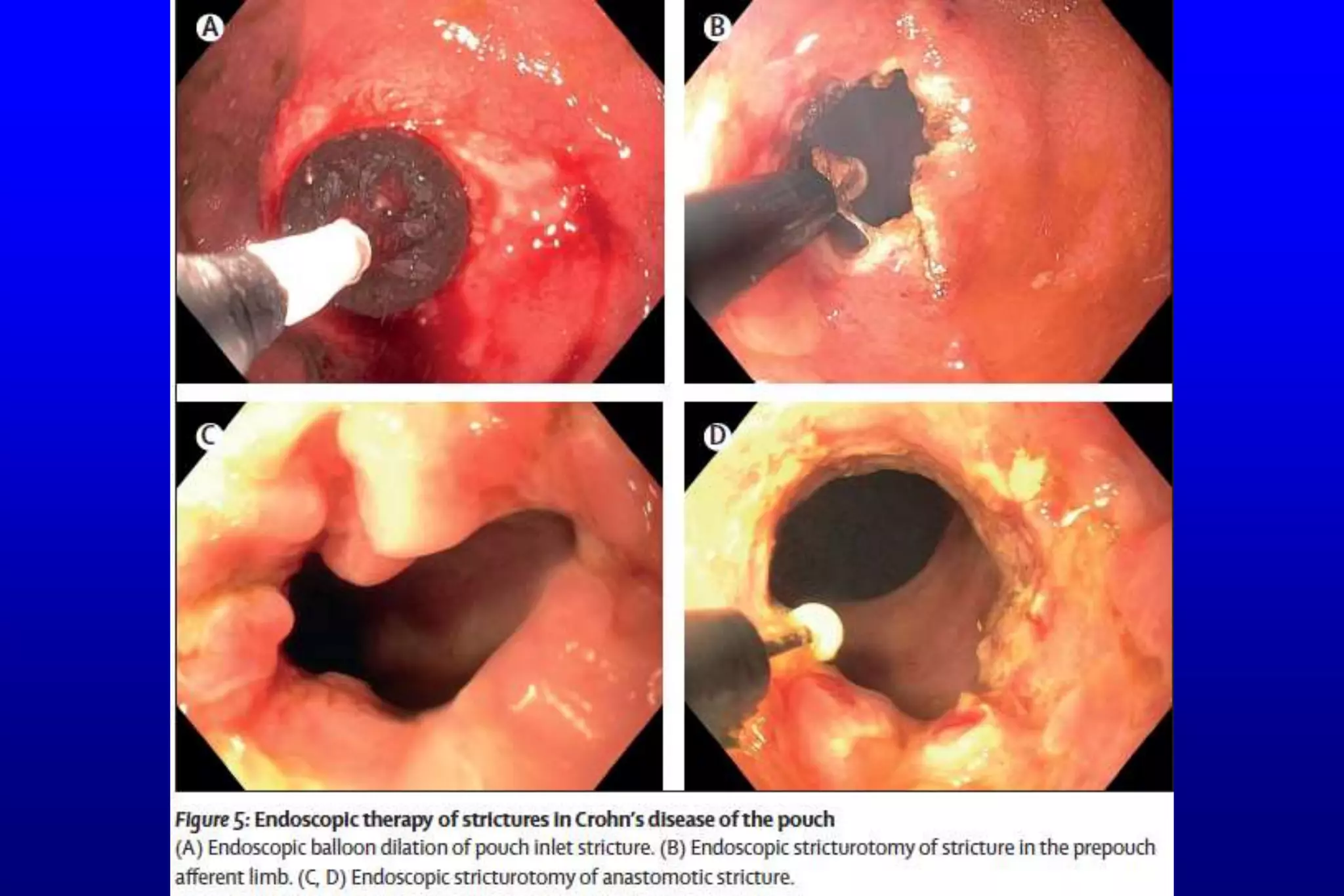
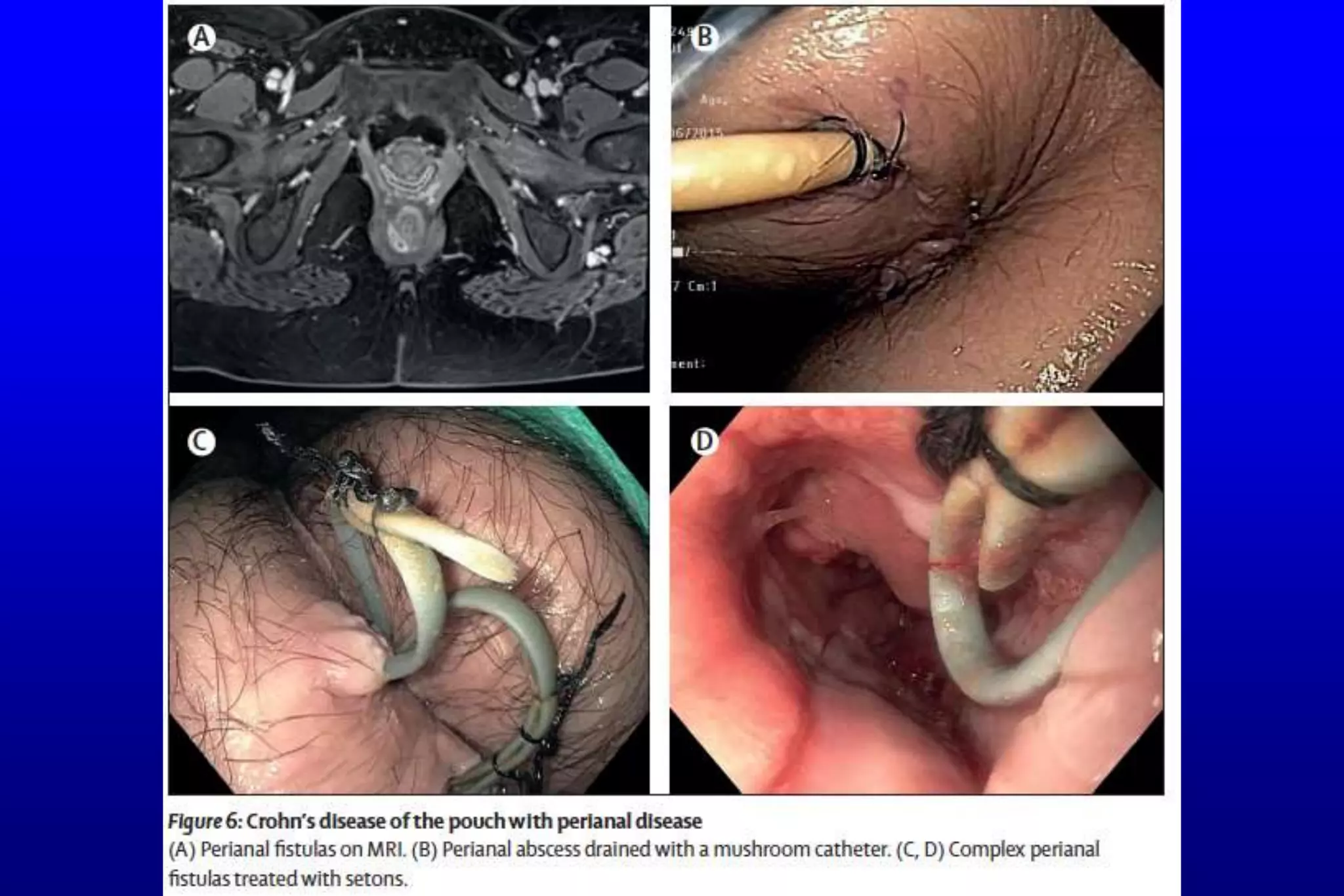
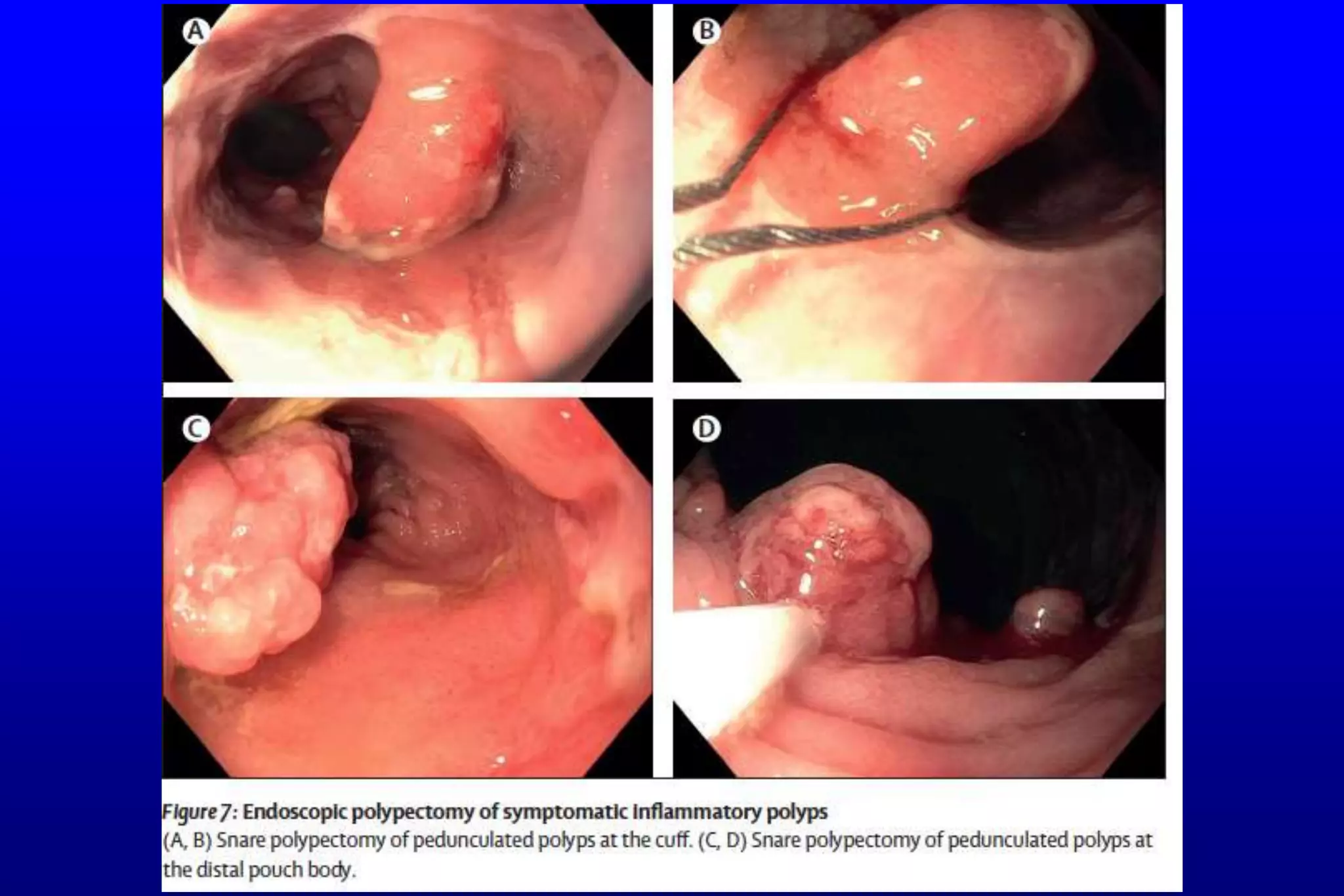
This document summarizes a journal club meeting on inflammatory disorders that can occur after restorative proctocolectomy with ileal pouch–anal anastomosis (IPAA). Pouchitis, Crohn's disease of the pouch, cuffitis, polyps, and extraintestinal manifestations are common inflammatory disorders. Acute pouchitis is usually treated with antibiotics, while chronic pouchitis may require biologics or anti-inflammatory therapies. Crohn's disease of the pouch is typically managed with biologics and endoscopic or surgical interventions for complications. The treatment of other disorders depends on their specific causes.









































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)












