Download to read offline

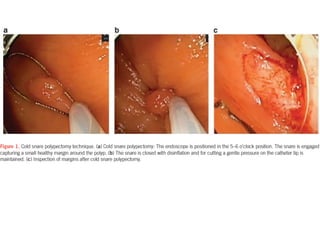

1. Cold snare resection is as effective and safe as hot snare resection for removing polyps up to 10mm in size. A dedicated cold snare using a gentle "push and cut" technique helps obtain a healthy tissue margin. 2. Incomplete resection rates of polyps removed by cold snare are lower than rates for hot snare resection, especially for polyps larger than 5mm. However, more evidence is still needed to establish the efficacy and safety of cold snare for larger polyps. 3. Future randomized controlled trials are needed to compare the effectiveness and safety of hot and cold snare resection, especially for polyps greater than 5mm, and to determine optimal techniques and outcomes.











































































































