Downloaded 25 times



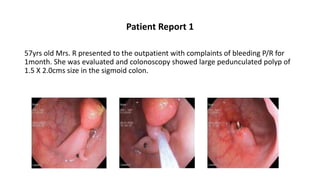




Endoscopic removal of colonic polyps is the standard care for managing colorectal cancer, which is a leading cause of cancer deaths globally. The document outlines two patient cases involving large colonic polyps treated by endoscopic polypectomy, detailing techniques and post-procedure follow-up protocols to manage complications and recurrence rates. It emphasizes the importance of follow-up examinations and provides the contact information for a hospital specializing in such procedures.



































































