Downloaded 770 times












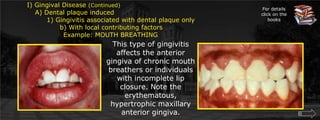

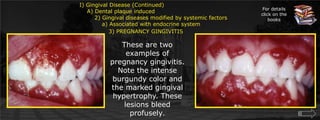
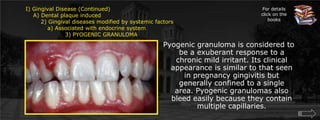
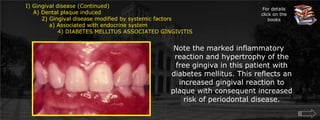


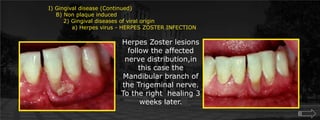

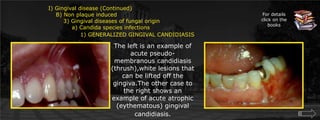

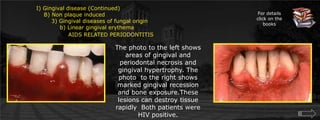
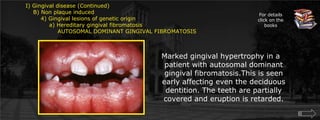

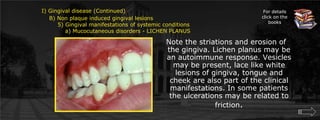
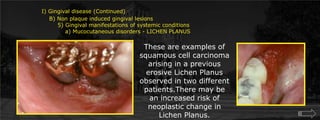
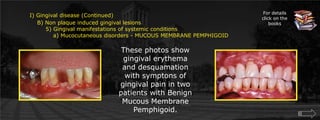



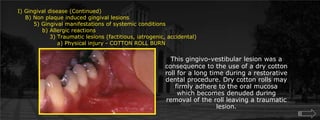
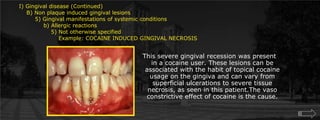
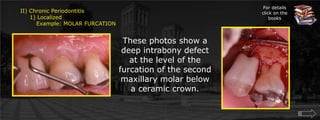
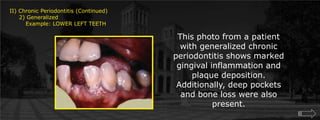









This document provides a classification system for periodontal pathology, dividing it into gingival diseases and periodontitis. It describes various forms of gingival disease including those induced by dental plaque, modified by systemic factors like pregnancy or diabetes, drug-induced forms from medications like phenytoin, and non-plaque induced lesions from conditions such as linear gingival erythema. It also outlines different types of periodontitis including chronic, aggressive, periodontitis associated with systemic diseases, necrotizing forms, abscesses, and lesions associated with endodontic problems. Developed deformities and occlusal trauma are additionally discussed.



















































































