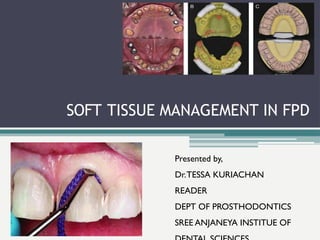
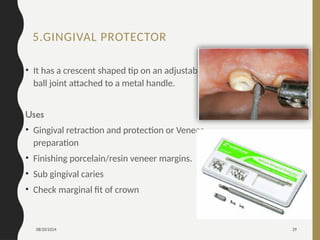
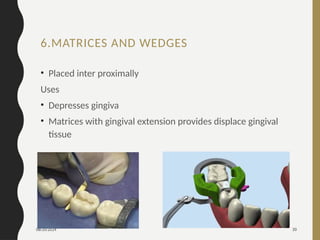
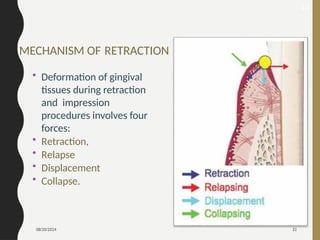
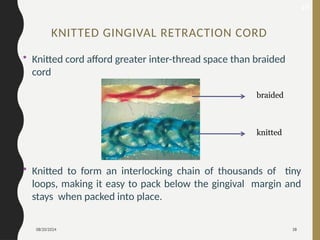
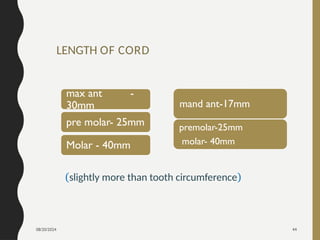
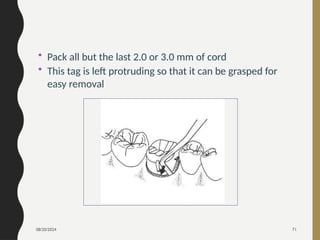
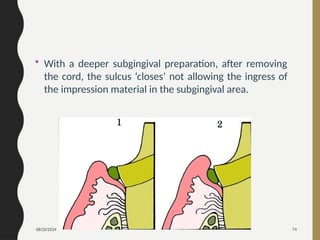
The document outlines various methods and techniques for soft tissue management in fixed prosthodontics, emphasizing the importance of effective gingival retraction for achieving optimal impressions and restorations. It categorizes retraction methods into mechanical, chemomechanical, and surgical techniques, detailing specific tools and products used in the process. The document also covers the pre-retraction assessment of gingival health and the desirable characteristics of retraction cords.