Downloaded 13 times



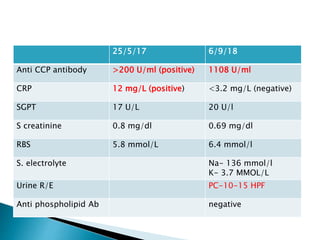
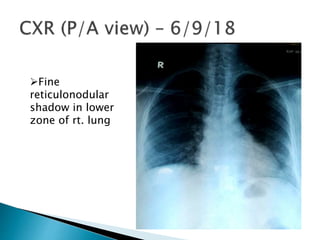
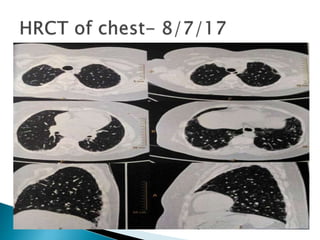

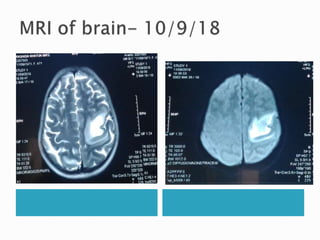
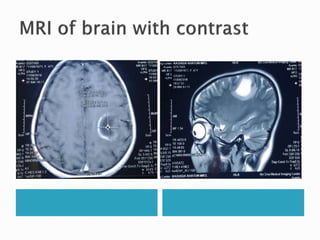
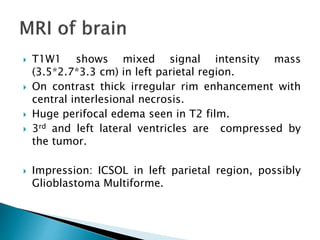


A 47-year-old homemaker presented with sudden weakness in her right upper limb, later diagnosed with rheumatoid arthritis and interstitial lung disease. Her treatment included methotrexate, which was stopped due to side effects, and she currently remains on salfasalazine and leflunomide. Imaging revealed a mass in the left parietal region suggestive of glioblastoma multiforme, alongside her existing conditions.









































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







