Gastro Intestinal Tract
•
73 likes•7,620 views

This document discusses the gastrointestinal tract and its components. It describes the structure and function of the oral cavity, esophagus, stomach, small intestine, large intestine, salivary glands, pancreas, liver, and their roles in digestion. Diagrams and histology slides of these organs are also included to illustrate their anatomical features. The document is presented by Prof. Dr. R.R. Deshpande and provides contact information.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Gastro Intestinal Tract
Similar to Gastro Intestinal Tract (20)
More from rajendra deshpande
More from rajendra deshpande (20)
Recently uploaded
Recently uploaded (20)
Gastro Intestinal Tract
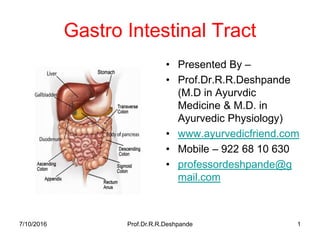
- 1. Gastro Intestinal Tract • Presented By – • Prof.Dr.R.R.Deshpande (M.D in Ayurvdic Medicine & M.D. in Ayurvedic Physiology) • www.ayurvedicfriend.com • Mobile – 922 68 10 630 • professordeshpande@g mail.com 7/10/2016 Prof.Dr.R.R.Deshpande 1
- 2. 7/10/2016 Prof.Dr.R.R.Deshpande 27/10/2016 Prof.Dr.R.R.Deshpande 2 Sharir Kriya -- Paper 1 –Part B –Point 5 • Presented By – • Prof.Dr.R.R.Deshpande (M.D in Ayurvdic Medicine & M.D. in Ayurvedic Physiology) • www.ayurvedicfriend.com • Mobile – 922 68 10 630 • mailme.drrrdeshpande@rediffmail.com
- 3. Sharir Kriya Paper 1-Part B –Set 2 • Presented By – • Dr.R.R.Deshpande • Prof & HOD • CARC ,Pune 44 7/10/2016 Prof.Dr.R.R.Deshpande 3
- 4. 7/10/2016 Prof.Dr.R.R.Deshpande 47/10/2016 Prof.Dr.R.R.Deshpande 4 Sharir Kriya Hand Book – 1st to last year BAMS • Best for Fast Revision • Paper 1,Paper 2 • Practicals • Instruments • Histology • IMP Schlok • All basics of Dodha,Dhatu & Mala
- 5. 7/10/2016 Prof.Dr.R.R.Deshpande 57/10/2016 Prof.Dr.R.R.Deshpande 5 Sharikriya Paper Practical Book • As per Very New Syllabus formed By CCIM IN 2012 • Ayurvedic Practicals like Prakruti,sara,Agni • Modern Haematological Practicals • CNS & CVS Examination
- 6. 7/10/2016 Prof.Dr.R.R.Deshpande 67/10/2016 Prof.Dr.R.R.Deshpande 6 Clinical Examination • Systemic Examination of 8 systems • Ayurvedic Srotas Examination • Clinical significance of Lab Tests & Radiology,USG,2D Echo
- 7. 7/10/2016 Prof.Dr.R.R.Deshpande 77/10/2016 Prof.Dr.R.R.Deshpande 7 Sharir Kriya Paper 1 • Book in English • Total CCIM Syllabus covered • Chaukhamba Sanskrit Pratisthan Publication • Popular Nationwide & In Germany also • Dosha & Prakruti
- 8. 7/10/2016 Prof.Dr.R.R.Deshpande 87/10/2016 Prof.Dr.R.R.Deshpande 8 Sharir Kriya Paper 2 • Book in English • Total CCIM Syllabus covered • Chaukhamba Sanskrit Pratisthan Publication • Popular Nationwide & In Germany also • Dhatu,Mala
- 9. 7/10/2016 Prof.Dr.R.R.Deshpande 9 Prof.Dr.Deshpande’s Popular Links on Internet • Just Start Internet on Desk top or Lap top or on your mobile . Copy Following Link & Paste as Web address –URL • http://www.youtube.com/user/deshpande1 959 • http://www.slideshare.net/rajendra9a/ • http://www.mixcloud.com/jamdadey/ 7/10/2016 Prof.Dr.R.R.Deshpande 9
- 10. 7/10/2016 Prof.Dr.R.R.Deshpande 10 Prof.Dr.Deshpande’s Popular Links on Internet • Just Start Internet on Desk top or Lap top or on your mobile . Copy Following Link & Paste as Web address –URL • http://professordeshpande.blogspot.in • http://professordrdeshpande.blogspot.in/ • http://www.mixcloud.com/rajendra- deshpande • https://soundcloud.com/professor- deshpande 7/10/2016 Prof.Dr.R.R.Deshpande 10
- 11. 7/10/2016 Prof.Dr.R.R.Deshpande 11 Digestion • The food, after ingestion, passes along the various parts of the digestive tract --- • Where it is converted into simple absorbable constituents.
- 13. Rectum & Anus 7/10/2016 13Prof.Dr.R.R.Deshpande
- 14. 7/10/2016 Prof.Dr.R.R.Deshpande 14 Functional anatomy of GIT • Important parts of digestive tract • 1) Oral cavity 2) Pharynx • 3) Oesophagus • 4) Stomach • 5) Small intestine (Duodenum, Jejunum & Ileum) • 6) Large intestines (Caecum, ascending colon, transverse colon, descending colon, iliac colon, sigmoid colon, rectum & anus) • The salivary glands, liver & pancreas are also developmentally associated with alimentary canal.
- 16. 7/10/2016 Prof.Dr.R.R.Deshpande 16 Structure of Digestive Tract • 1) Oral cavity is lined by stratified epithelium. • 2) From oesophagus onwards, the digestive tract on transverse section show 4 layers - • Serous layer (outermost) • Muscular layer consists of longitudinal & circular muscle fibers • Submucous layer • Mucous layer.
- 17. 7/10/2016 Prof.Dr.R.R.Deshpande 17 Structure & appearance of teeth • A tooth consists of a crown, a neck & a root. • The crown is the portion projecting above the gum. • The slight constriction where it is surrounded by the gum margin is the neck & the part buried in the alveolus of the jaw is the root
- 18. 7/10/2016 Prof.Dr.R.R.Deshpande 18 Structure & appearance of teeth • The main mass of the tooth consists of a substance called dentine, a very hard material which resembles bone. • The exposed portion of the tooth is covered with a thin layer of enamel, which is even stronger than dentine.
- 19. 7/10/2016 Prof.Dr.R.R.Deshpande 19 Structure & appearance of teeth • The interior of a tooth is hollow & is called the pulp cavity. • This contains soft connective tissue, small blood vessels & nerves, which enter the root of the tooth through a fine canal.
- 20. 7/10/2016 Prof.Dr.R.R.Deshpande 20 Structure & appearance of teeth • The teeth are firmly fixed in the alveoli of the jaw --- • By a special calcified cement substance & a strong layer of connective tissue called the periodontal membrane
- 21. 7/10/2016 Prof.Dr.R.R.Deshpande 21 Structure & appearance of teeth • The incisor teeth have a crown consisting of a sharp cutting edge, & a single pointed root. • • The canines have a crown, which terminates in a point & a single root.
- 22. Structure & appearance of teeth • The premolars have a single root & a crown consisting of 2 elevations or cusps (which explains why they are sometimes called bicuspids) • The molars have a square - shaped crown with 4 cusps. The upper molars possess 3 roots, the lower 2 roots. 7/10/2016 Prof.Dr.R.R.Deshpande 22
- 23. 7/10/2016 Prof.Dr.R.R.Deshpande 23 Structure & appearance of teeth • The incisors are the sharp cuttings, or biting, teeth situated in front. • To the lateral side of the incisors are the canine teeth (eye teeth), used for grasping. • Behind the canines are the premolars & the molars, or grinding teeth.
- 24. 7/10/2016 Prof.Dr.R.R.Deshpande 24 Types & Number of Teeth
- 25. 7/10/2016 Prof.Dr.R.R.Deshpande 25 Structure of Tooth
- 26. 7/10/2016 Prof.Dr.R.R.Deshpande 26 Shapes of Human teeth
- 27. 7/10/2016 Prof.Dr.R.R.Deshpande 27 1) Oesophagus • Extends from pharynx to cardiac orifice & is 2 cm. in diameter
- 29. 7/10/2016 Prof.Dr.R.R.Deshpande 29 Stomach • Stomach has a J - shaped structure. • It communicates above with oesophagus through cardiac orifice & below with duodenum through pyloric orifice. • It’s main parts are fundus, body & pylorus. •
- 31. Stomach Histology • Slide - Serosa, muscularis (longitudinal-circular-oblique • muscle layer), submucosa, mucosa, gastric pits, gastric • glands, goblet cells. • Serosa - Peritoneum, • Submucosa - Arteries, veins, nerves; • Mucosa - Simple columnar epithelium. • 4 types of gastric glands • • Chief or Zymogenic - pepsinogen, • • Parietal - HCl and gastric intrinsic factor, • • Mucous - Mucus, • • Enteroendocrine - Stomach gastrin • (Gastric pits are deeper in pyloric part) 7/10/2016 31Prof.Dr.R.R.Deshpande
- 32. Stomach • The body is bound by lesser & greater curvatures. • The lesser curvature extends from cardiac end to incisuria angularis. • • The greater curvature extends from fundus to pylorus 7/10/2016 Prof.Dr.R.R.Deshpande 32
- 33. 7/10/2016 Prof.Dr.R.R.Deshpande 33 Small Intestine • Extend from gastric pyloric orifice onwards up to ileo colic junction which is guarded with ileocolic sphincter. • Small intestines are about 6. 5 meters in length, first 20 - 25 cm portion is formed by the duodenum, about 2/5 th by jejunum & 3/5th by ileum.
- 34. Small Intestine • The duodenum & jejunum are mainly concerned with digestive processes,-- • While the main function of ileum is absorption (Hence it is richly supplied with villi) 7/10/2016 Prof.Dr.R.R.Deshpande 34
- 35. Small Intestine Anatomy 7/10/2016 35Prof.Dr.R.R.Deshpande
- 36. Small Intestine Histology 7/10/2016 36Prof.Dr.R.R.Deshpande
- 37. Histology of Small Intestine • Slide - Serous, muscularis (Longitudinal, circular),submucosa, mucosa, villi, crypts of Liberkuhn • Mucosal folds = villi. Villi - Lined with ciliated columnar epithelium. • At base of mucosa - Intestinal glands (Crypts of Liberkuhn). • In mucosa - Goblet cells, Enteroendocrine glands. 7/10/2016 37Prof.Dr.R.R.Deshpande
- 38. 7/10/2016 Prof.Dr.R.R.Deshpande 38 Large Intestine • It is about 1. 5 meters in length & is called as large intestines because, it has large diameter than small intestines • • It extends from ileo - colic junction to anus.
- 39. Large Intestine Anatomy 7/10/2016 39Prof.Dr.R.R.Deshpande
- 40. Large Intestine • Its different parts are ---- • caecum (and appendix), • ascending colon, hepatic flexure, transverse colon, splenic flexure, descending colon, iliac colon, • sigmoid colon & anal sphincter (involuntary in function) • & at the lower end at anal canal is external anal sphincter (Voluntary in function) 7/10/2016 Prof.Dr.R.R.Deshpande 40
- 41. Large Intestine Histology 7/10/2016 41Prof.Dr.R.R.Deshpande
- 42. Histology of Large Intestine • Slide - Serous, muscularis, submucosa, mucosa (villi- absent) • Mucosa - Few Intestinal glands, but goblet cells and lymphatic nodules - numerous. 7/10/2016 42Prof.Dr.R.R.Deshpande
- 43. Comparison of Small & Large Intestine Histology 7/10/2016 43Prof.Dr.R.R.Deshpande
- 44. 7/10/2016 Prof.Dr.R.R.Deshpande 44 Important glands in connection with digestion • 1) Salivary glands • Salivary glands secrete saliva. 3 pairs of salivary glands are • submaxillary (submandibular) glands open through Wharton duct at side of frenum of tongue at the floor of the mouth • parotid gland - open through stenson’s duct to opposite the 2nd upper molar tooth, • sublingual glands open through ducts of Rivinus (10 - 12 ducts) at side of frenum of tongue, at the floor of the mouth.
- 45. Anatomy of Salivary Glands 7/10/2016 45Prof.Dr.R.R.Deshpande
- 46. 7/10/2016 Prof.Dr.R.R.Deshpande 46 2) Pancreas • It is an elongated racemose gland; situated at posterior wall of the abdomen. • Pancreas secretes pancreatic juice & also it has alpha & beta cells of islets of Langerhans. • The beta cells secrete insulin & alpha cells glucagon. • Pancreatic juice contains digestive enzymes (trypsin, chymotrypsin)
- 47. 7/10/2016 Prof.Dr.R.R.Deshpande 47 Biliary Tract & Pancreas
- 50. Histology of Pancreas 7/10/2016 50Prof.Dr.R.R.Deshpande
- 51. Histology of Pancreas • Slide - Pancreatic acini, Islets of Langerhans - Alpha and beta cells. • Pancreas - Both Exocrine and Endocrine, Divided into Lobes, • Pancreatic Acini → secrets Pancreatic Juice, Cells of Islets of • Langerhans → Beta cells - Insulin, Alpha cells → Glucagon. 7/10/2016 51Prof.Dr.R.R.Deshpande
- 52. 7/10/2016 Prof.Dr.R.R.Deshpande 52 Liver • It is an important & essential metabolic organ of the body. • The liver cells secrete bile. • Although bile is not a digestive juice, in its strict sense, it is helpful, rather essential, for digestion & absorption of fats, hence it is considered along with digestive juices.
- 55. Liver Histology 2 7/10/2016 55Prof.Dr.R.R.Deshpande
- 56. Histology of Liver • Slide --- Central vein, Hepatocytes, Branch of Hepatic Artery and portal vein + Bile duct; Kupffer cells, sinusoid, Bile canaliculi. • Liver - Largest gland - covered with connective tissue sheath (Glisson’s sheath) • Bile - Formed inside the Hepatocytes. • Sinusoids - Contain R.E cells (Kupffer cells) • Functions of Liver -- Formation of Bile, phagocytosis by Kupffer cells, Vitamin-Ironfat • storage. 7/10/2016 56Prof.Dr.R.R.Deshpande
- 57. 7/10/2016 Prof.Dr.R.R.Deshpande 57 Gall bladder • It stores & concentrates the bile received from liver via hepatic duct. • Through cystic duct it joins hepatic duct to form common bile duct, which in turn joins pancreatic duct to form ampulla of Vater guarded by “Sphincter of Oddi”, which relaxes after fatty meal to allow drainage of bile in the duodenum
- 58. 7/10/2016 Prof.Dr.R.R.Deshpande 58 Structure of Gall bladder
- 59. Liver ,Gall Bladder ,Pancreas 7/10/2016 59Prof.Dr.R.R.Deshpande
- 60. 7/10/2016 Prof.Dr.R.R.Deshpande 60 Functions of Liver -1 • 1) In Connection With Blood & Circulation • RBC formation, in foetal life. • RBC destruction in adult life. • Store house of blood & regulates blood volume. • Manufactures prothrombin & fibrinogen & thus essential for clotting. Mast cells form heparin & prevent intravascular clotting.
- 61. 7/10/2016 Prof.Dr.R.R.Deshpande 61 Functions of Liver -2 • Related to activity of its R.E. system in immune mechanism. • It transfers blood from portal to systemic circulation. • Manufactures all plasma proteins. • Stores iron, haematinic factor known as Vit. B12 & copper & thus helps in the formation of red cells & haemoglobin. • Hepatic & portal circulation control
- 62. 7/10/2016 Prof.Dr.R.R.Deshpande 62 Functions of Liver - 3 • 2) Manufactures Bile • Bile is secreted continuously from the liver cells & stored in the gall bladder. Bile contains water, total solid, mucin & pigments, neutral fat, fatty acids, phospholipids, cholesterol & inorganic ions. • Bile acids in conjugation with glycerin & taurine form the compounds - bile salts - glycochloric acid & taurocholic acid respectively. Bile salts perform important function of emulsification of fats
- 63. 7/10/2016 Prof.Dr.R.R.Deshpande 63 Functions of Liver - 4 • 3) Relation With Carbohydrate Metabolism • Converts non glucose monosaccharides into glucose. • Converts lactic acid, pyruvic acid & glycerol into glucose & also glycogen. • Stores carbohydrates in the form of glycogen. • Takes part in blood sugar regulation.
- 64. 7/10/2016 Prof.Dr.R.R.Deshpande 64 Functions of Liver - 5 • Manufactures fats from carbohydrates etc. • Alcohol metabolism - The liver is the main seat of alcohol metabolism. The direct effect of alcohol may be alcoholic fatty liver, which is the cause of increased hepatic fatty acid oxidation.
- 65. 7/10/2016 Prof.Dr.R.R.Deshpande 65 Functions of Liver - 6 • 4) Relation With Fat Metabolism • It stores fat. • It helps in the oxidation of fat, releasing energy in the form of A.T.P. • Site of synthesis of cholesterol from acetate.
- 66. 7/10/2016 Prof.Dr.R.R.Deshpande 66 Functions of Liver - 7 • Synthesizes fats from carbohydrates & proteins. • It is the seat of ketone body formation. • Unused free fatty acid (FFA) released from fat depot is converted to triglycerides & other lipids to meet energy requirement
- 67. 7/10/2016 Prof.Dr.R.R.Deshpande 67 Functions of Liver - 8 • In a carbohydrate deficiency, the fat metabolism in the liver is increased & fat is partially converted to glucose or glycogen. • • Fat soluble vitamins, eg. - A, D, E & K are stored here
- 68. 7/10/2016 Prof.Dr.R.R.Deshpande 68 Functions of Liver - 9 • 5) Relation With Protein Metabolism • Synthesis of some amino acids takes place here. • Plasma proteins are manufactured here except immune globulin. • Main seat of urea & uric acid formation. • It is the seat of specific dynamic action of protein. • It is the seat of nitrogen metabolism
- 69. 7/10/2016 Prof.Dr.R.R.Deshpande 69 Functions of Liver - 10 • 6) Hormone Metabolism • Reduces the circulating adrenal cortical & sex hormones by degradation & conjugation. • Inactivation of insulin, glucageon, anti - diuretic hormones (ADH) & anterior pituitary tropic hormones etc. occur here.
- 70. 7/10/2016 Prof.Dr.R.R.Deshpande 70 Functions of Liver - 11 • 7) Relation With Vitamins • Manufactures prothrombin with the help of vit. K. • It forms vit. A from carotene & stores vit. A & D. • Chronic liver disease is always associated with folic acid deficiency. • The liver is the principal storage organ for vit. B12.
- 71. 7/10/2016 Prof.Dr.R.R.Deshpande 71 Functions of Liver - 12 • 8) Excretory Functions • Certain heavy metals are temporarily fixed by the liver cells, which are then excreted in the bile. • Various toxins, bacteria & drugs are excreted through bile. • Cholesterol & bile pigments are excreted in the bile.
- 72. 7/10/2016 Prof.Dr.R.R.Deshpande 72 Functions of Liver - 13 • 9) Detoxicating & Protective Functions • The liver is the site of detoxication of different toxic substances either produced in the body or taken along with food. • 10) Takes Part In Heart Regulation • The liver produces a large amount of heat & takes part in heart regulation.
- 73. 7/10/2016 Prof.Dr.R.R.Deshpande 73 Functions of Liver - 14 • 11) It is also responsible for the liberation of a depressor principle. • 12) It is the store house of Fe, fat soluble vitamins, glycogen, labile protein, fat etc.
- 74. 7/10/2016 Prof.Dr.R.R.Deshpande 74 Digestive system • Functional term that differentiate between dead & living body i.e. metabolism. • 1) Accumulation or storage of energy is called as anabolism • 2) Loss of energy - catabolism • Due to catabolism, our body is able to perform physical & mental activities.
- 75. 7/10/2016 Prof.Dr.R.R.Deshpande 75 Digestive system • Let us try to understand, how energy enters in living body, how it get stores, or loosed by body (Energy turn over) ? • The human body gets the energy from food. Actually sunrays, which are electromagnetic radiation, are the true source of energy in world. • Human living cells do not have the capacity for absorbing energy of sun rays & form the food by themselves.
- 76. 7/10/2016 Prof.Dr.R.R.Deshpande 76 Digestive system • Plants capacity of absorbing energy of sun rays is mainly due to green pigments called as chlorophyll. • Chlorophyll molecules take CO2 & water from air & soil respectively & they are tied together to form a compound carbohydrate. • This binding function is done with the help of energy from sunrays. • So radiation energy is converted into material form of food, which a human being can use as a source of energy for performing physical & mental activities.
- 77. 7/10/2016 Prof.Dr.R.R.Deshpande 77 Plants form Glucose molecules
- 78. 7/10/2016 Prof.Dr.R.R.Deshpande 78 In Plant -- Polysaccharides • Glucose is called as monosaccharides (Glucose). • In plant, chain of glucose molecules is formed (to store more energy) which are called as polysaccharides
- 79. 7/10/2016 Prof.Dr.R.R.Deshpande 79 Proximal Principles of Food • 1) Our food is mainly made up of polysaccharides or complex carbohydrate • 2) Binding carbohydrates with nitrogen molecule, higher energy molecules of proteins are formed. • 3) Fats are very high energy molecules which are formed by combining carbohydrates with fatty acid (COOH)
- 80. 7/10/2016 Prof.Dr.R.R.Deshpande 80 Complex to Simpler molecules • For performing body activities, the food that is complex molecules should be broken up for absorption purpose. In digestive system, due to action of different enzymes & chemicals (Bile, HCL) complex molecules break up & simpler molecules are formed • Carbohydrates → Glucose • Protein → Amino acid • Fats → Fatty acid & glycerol
- 81. 7/10/2016 Prof.Dr.R.R.Deshpande 81 Functions of CVS & RS • This simpler molecule should reach to different cells of body. This transport is done through blood. Proper blood circulation is maintained by cardiovascular system. • These molecules are oxidized with oxygen to liberate energy. O2 for oxidation is provided by respiratory system.
- 82. 7/10/2016 Prof.Dr.R.R.Deshpande 82 Role of systems • Waste product formed during oxidation are carried back to kidneys, lungs, skin through excretory system. • The total regulation & co - ordination of all these metabolic activities is done by nervous system & endocrine system
- 83. 7/10/2016 Prof.Dr.R.R.Deshpande 83 Physiology = GOD • Physiology is nothing but to understand the concept of GOD • i.e. energy turn over → • Genesis + Operation + Destruction
- 84. 7/10/2016 Prof.Dr.R.R.Deshpande 84 5 Secretions & 5 Movements
- 85. 7/10/2016 Prof.Dr.R.R.Deshpande 85 How to study ? • To study the physiological aspect, we have to consider --- • Composition, • Function & • Regulation.
- 86. 7/10/2016 Prof.Dr.R.R.Deshpande 86 1) Salivary secretions • Parotid 20% Serous • Sub mandibular 70% Mixed • Sublingual 10% Mucus
- 87. 7/10/2016 Prof.Dr.R.R.Deshpande 87 Structure of Salivary glands
- 88. 7/10/2016 Prof.Dr.R.R.Deshpande 88 Salivary secretions • Secretions • 1) Salivary amylase (Ptyline) • 2) Mucin • 3) Na+, K+, HCO3- • 4) Blood group antigen
- 89. 7/10/2016 Prof.Dr.R.R.Deshpande 89 Functions of Salivary Glands - 1 • 1) Cleaning of oral cavity • 2) Prevents caries, antiseptic action (due to Lysozyme) • 3) Alkaline medium & so Ca++ deposited on teeth • 4) Formation of bolus • 5) Lubrication of bolus
- 90. 7/10/2016 Prof.Dr.R.R.Deshpande 90 Functions of Salivary Glands- 2 • 6) Softening of food • 7) Boiled starch.
- 91. 7/10/2016 Prof.Dr.R.R.Deshpande 91 Functions of Salivary Glands - 3 • 8) Helps in speech • 9) Taste perception • 10) Neutralizes acidity in stomach • • 11) Water balance
- 92. 7/10/2016 Prof.Dr.R.R.Deshpande 92 Regulation of Salivary secretions • Regulation = Nervous, hormonal • Salivary gland is exception for above route. Only nervous regulation is done by parasympathetic nerve. • 7th cranial nerve (facial) → submandibular, sublingual • 9th cranial nerve (glossopharyngeal) → parotid
- 93. 7/10/2016 Prof.Dr.R.R.Deshpande 93 Phases • 1) Cephalic phase • 2) Oral phase • 3) Gastric phase
- 94. 7/10/2016 Prof.Dr.R.R.Deshpande 94 Salivary secretions • 1) Tubo acinar glands • Acini - lobule - columnar epithelium manifacting of enzymes • Duct - cuboidal epithelium - secretes bicarbonates - HCO3- • 2) Blood group determination from saliva is important in medicolegal cases.
- 95. 7/10/2016 Prof.Dr.R.R.Deshpande 95 Salivary secretions • 3) Decomposition of carbohydrates forms acid. • This acid medium will dissolves the calcium & caries of teeth will develop. • To avoid this, function of saliva (killing of microorganism) is important
- 96. 7/10/2016 Prof.Dr.R.R.Deshpande 96 Salivary secretions
- 97. 7/10/2016 Prof.Dr.R.R.Deshpande 97 Salivary secretions • In the mouth partial digestion of carbohydrates take place as follows – Starch is converted → Dextrin & maltose • Polysaccharide → Diasaccharide
- 98. 7/10/2016 Prof.Dr.R.R.Deshpande 98 Salivary secretions • This digestion is completed by pancreatic amylase. • The importance of proper chewing food lies in above concept. • If we do not give the proper time for action of salivary amylase there will be burden on Pancreas. • Naturally functional capacity of Pancreas will be reduced at early stage of life & patient will land into Diabetes mellitus.
- 99. 7/10/2016 Prof.Dr.R.R.Deshpande 99 Salivary secretions • 5) Parasympathetic nerves are “secretomotor” in action in G.I. tract i.e. they will increase secretion & also motility. • These nerves stimulate acini.
- 100. 7/10/2016 Prof.Dr.R.R.Deshpande 100 3 Phases • a) Cephalic phase - saliva increases after thought of food or sight of food. • b) Oral phase - It is most important. It is due to contact of food with Taste buds. Signals pass to brain from these Taste buds (Gustatory pathway) • c) Gastric phase - Presence of food in stomach increases salivary secretions. After eating spicy food, saliva increases, as a protective mechanism
- 101. 7/10/2016 Prof.Dr.R.R.Deshpande 101 Salivary secretions • 6) a) Mumps virus has specific affinity to salivary cells. • b) Hyperthyroidism - serum calium level increases. • Hence stone formation takes place in may places in body. • (Gall stones, salivary stones, & pancreatic stones)
- 102. 7/10/2016 Prof.Dr.R.R.Deshpande 102 Gastric Secretion
- 103. 7/10/2016 Prof.Dr.R.R.Deshpande 103 Gastric Secretion • Secretions – • 1) HCL / NaCl / KCl • 2) Intrinsic factor (IF) • 3) Pepsinogen • 4) Mucin • 5) Enzymes - Pepsinogen, Renin
- 104. 7/10/2016 Prof.Dr.R.R.Deshpande 104 Gastric Secretion - Functions • 1) HCL - Antiseptic • Activation of pepsinogen • Provides acidic medium for action of enzymes • Iron & calcium absorption
- 105. 7/10/2016 Prof.Dr.R.R.Deshpande 105 Gastric Secretion - Functions • 2) Digestive • c) Intrinsic factor is essential for absorption of Vit B12 factor • d) Mucin - Protects mucosa against acidity
- 106. 7/10/2016 Prof.Dr.R.R.Deshpande 106 Regulation of Gastric Secretion
- 107. 7/10/2016 Prof.Dr.R.R.Deshpande 107 Gastric Secretion Phases • Phases – • 1) Cephalic • 2) Gastric • 3) Intestinal
- 108. 7/10/2016 Prof.Dr.R.R.Deshpande 108 Pathology of HCL secretion
- 109. 7/10/2016 Prof.Dr.R.R.Deshpande 109 Pepsinogen to Pepsin • 1) Salivary glands are 3 in number but gastric glands are many. • 2) Pepsinogen (Gen = genesis) is inactivated form. Due to HCl only, it is converted into active form i.e. pepsin • 3) Ferric (Fe3+) cannot be absorbed. Due to effect of HCl it is converted into ferrous form (Fe++) which can be absorbed.
- 110. 7/10/2016 Prof.Dr.R.R.Deshpande 110 Vitamin C with Iron • 4) Ferrous iron can only be absorbed & this form is needed for hemoglobin formation. • Iron preparation is always given with vitamin C (ascorbic acid) vitamin C keeps iron in ferrous form. • 5) Proteins that we eat are polypeptide (amino acid linkage) Due to pepsin break down of this linkage takes place
- 111. 7/10/2016 Prof.Dr.R.R.Deshpande 111 Mucin prevents ulcer • 6) Mucin is alkaline & sticky. It forms the buffer coat on gastric mucosa. • In gastric mucosa rapid mitosis takes place. • Above 2 facts prevent ulceration in stomach (Peptic ulcer) • 99% of ulcers occur in duodenum because there is no protective mechanism.
- 112. 7/10/2016 Prof.Dr.R.R.Deshpande 112 Mid Night Pain • 7) Presence of food & distention of stomach causes afferent sensation. Hence vagotomy is the surgical treatment in peptic ulcer (afferent & efferent both are cut) • 8) In duodenum ulcers mid night pain is common (i.e. after 2 ½ to 3 hr. after eating pain starts. That means when food comes in duodenum from stomach pain starts.)
- 113. 7/10/2016 Prof.Dr.R.R.Deshpande 113 Gastric Emptying Time • 9) HCl maintains appetite hence hyper acidity patients eat frequently. In hyper acidity patient gastric emptying time is also shorter. • 10) Gastric moments are affected by type of food • More acidic food - fast emptying time • More carbohydrates or protein - faster emptying time
- 114. 7/10/2016 Prof.Dr.R.R.Deshpande 114 Fats delay Emptying Time • More fats - delayed emptying time • Reason - Due to fatty food CCK hormone is stimulated. This hormone inhibits gastrin, hence motility is reduced
- 115. 7/10/2016 Prof.Dr.R.R.Deshpande 115 Investigations • 11) For testing of stomach functioning following 3 tests can be done • Gastric analysis (Out dated) • Barium meal X - ray • Gastroscopy - by Gastroenterologist
- 116. 7/10/2016 Prof.Dr.R.R.Deshpande 116 Treatment for hyperacidity • 1) Milk neutralizes HCl → thus milk diet is important. • Anticholinergic drugs • 2) which block vaso vagal action. • 3) Histamine blocking drugs (H2 Receptor Blockers) • Tab omez (Omeprazole) - 1BD • Tab Histac - 1 BD • When there is pyloric stenosis (complication of ulcer) Surgical treatment is ‘gastrojejunostomy
- 117. 7/10/2016 Prof.Dr.R.R.Deshpande 117 3) Pancreatic secretion (Tubulo acinar gland) • 1) Trypsinogen • 2) Chymotrypsinogen • 3) P. Amylase • 4) Lipase • 5) Trypsin inhibitor • 6) HCO3 / Na & K
- 118. 7/10/2016 Prof.Dr.R.R.Deshpande 118 Function of Pancreatic secretion
- 119. 7/10/2016 Prof.Dr.R.R.Deshpande 119 Function of Pancreatic secretion
- 120. 7/10/2016 Prof.Dr.R.R.Deshpande 120 Pancreatic Enzymes • 1) Enterokinase enzyme is present in Duodenum (intestinal juice) • Which converts inactive enzyme (Trypsinogen) into active form (Trypsin) • 2) In pancreas, enzymes are not in active form - Due to trypsin inhibitor. • Enzymes get activated when they come in duodenum
- 121. 7/10/2016 Prof.Dr.R.R.Deshpande 121 Acute Pancreatitis • 3) When Trypsin inhibitor is absent Auto digestion of Pancrease takes place. • Exocrine & endocrine functions lost - which is irreversible. • This condition is called as Acute Pancreatitis. • This case is of acute abdomen. • Patient get severe stabbing pain in the epigastric region, referred to back. • Alcohol consumption is predisposing factor
- 122. 7/10/2016 Prof.Dr.R.R.Deshpande 122 4) Bile secretion • Bile is formed in Liver & • Stored in gall - bladder & • Through the bile duct it enters into duodenum
- 123. 7/10/2016 Prof.Dr.R.R.Deshpande 123 Bile -- Contents • i) Bile salts (Sodium taurocolate, Sodium glycolate) • ii) Bile pigments (Bilirubin & Biliverdin) • iii) Cholesterol (ester) • iv) HCO- 3 (Na & K)
- 124. 7/10/2016 Prof.Dr.R.R.Deshpande 124 Bile - Function • Emulsification of fats (Big fat molecules are broken down into smaller particles.) Hence surface area increases, so action of Lipase becomes easier) • Note - In urine examination test for Bile salt (Sulphur test) is based on this information.
- 125. 7/10/2016 Prof.Dr.R.R.Deshpande 125 Control of bile secretion & expulsion of bile from Gall bladder
- 126. 7/10/2016 Prof.Dr.R.R.Deshpande 126 Control of bile secretion & expulsion of bile from Gall bladder • Due to CCK hormone, Gall bladder contraction increases. • Note - Bile does not contain any enzyme • 1) But still it is very necessary for fat digestion (for action of Lipase enzyme) by emulsification of fat • 2) Pathologically - Gall stones can cause Obstructive jaundice • Gall stones are common in fat, fertile, female of forty complaining of flatulence. (Remember as ‘5 F’)
- 127. 7/10/2016 Prof.Dr.R.R.Deshpande 127 5) Intestinal Juice – Succus Entericus
- 128. 7/10/2016 Prof.Dr.R.R.Deshpande 128 Large intestinal functions 1 • 1) Absorption of H2O, electrolytes (Cl, HCO-3) • 2) Colonic bacteria - They are useful for production of Vit. B12 & Vit. K. These lactobacillus are the example of symbiosis. • Due to antibiotics these intestinal bacterial flora gets disturbed so antibiotics should be supplemented with vitamin tablets. • Buttermilk contains these lacto bacillus so this is best diet in patients of Colitis.
- 129. 7/10/2016 Prof.Dr.R.R.Deshpande 129 Large intestinal functions 2 • 3) Movements of large intestine push undigested food ahead into the rectum. • After filled with faecal matter signal goes through spinal cord to the brain
- 130. 7/10/2016 Prof.Dr.R.R.Deshpande 130 Large intestinal functions • Dorsal column sensory tract → Parital lobe → Frontal lobe → Motar centre of evacuation. • It will decide according to place & condition, whether to evacuate or not. • Then signal from pyramidal tract come to spinal cord. • • From spinal cord parasympathetic fibers contract rectum. • Through CNS motar signals to external sphincters are given, to open it.
- 131. 7/10/2016 Prof.Dr.R.R.Deshpande 131 Absorption through villi • Amino acids & glucose are absorbed into blood capillaries • Fatty acids are absorbed into lacteals (Lymph vessels)
- 132. 7/10/2016 Prof.Dr.R.R.Deshpande 132 Assimilation • Absorbed food is taken up by the protoplasm. • Then building up process is called ‘Assimilation’
- 133. 7/10/2016 Prof.Dr.R.R.Deshpande 133 Movements of GI tract • Deglutition • 1) Process of swallowing of food. • 2) Phases --- • i) Oral phase • ii) Pharyngeal phase • iii) Oesophageal phase.
- 134. 7/10/2016 Prof.Dr.R.R.Deshpande 134 i) Oral Phase • Masticated food is mixed with saliva. • Bolus is pushed back to pharynx, by movement of tongue. • This phase is voluntarily controlled by muscle of tongue. (Supplied by Hypoglossal nerve)
- 135. 7/10/2016 Prof.Dr.R.R.Deshpande 135 ii) Pharyngeal phase - Involuntary • Events are • a) Elevation of trachea. • b) Epiglottis falls on trachea, to close it. • c) Nasopharynx is closed by contraction of muscle of soft palate. • d) Pharyngo - oesophageal sphincter opens. • e) Vocal cords are approximated. • f) In all these events, respiration stops temporarily (Deglutition Apnoea)
- 136. 7/10/2016 Prof.Dr.R.R.Deshpande 136 Deglutition - Control • Reflex mechanism. • Presence of food in pharynx, stimulate touch receptors. Afferent impulses travel via 9th, 10th & 5th cranial nerves to the brain stem. • Deglutition center is situated in medulla. Efferent impulses come through 9th, 10th & 11th cranial nerves & bring about synchronized events of this phase
- 137. 7/10/2016 Prof.Dr.R.R.Deshpande 137 iii) Oesophageal Phase • Involuntary phase 2 components • a) Primary peristalsis - due to activity of pacemaker at pharyngo - oesophageal center. • • b) Secondary peristalsis - presence of food causes distention of oesophagus. • Afferent impulses travel via Vagus nerve. From Vagus center efferent impulses come via Vagus nerve & increase peristalsis.
- 138. 7/10/2016 Prof.Dr.R.R.Deshpande 138 Deglutition • When food reaches cardiac sphincter, it opens by receptive relaxation. • Food enters into stomach & sphincter closes. • This prevents regurgitation.
- 139. 7/10/2016 Prof.Dr.R.R.Deshpande 139 Deglutition - Pathology • Dysphagia - Difficulty in deglution • Main cause - Cancer of oesophagus. Also occurs in ‘Achalasia cardia - when cardiac sphincter is not relaxing properly. • Regurgitation of food from nose or into Trachea • (Causing coughing reflex) • This can happen if nerves are damaged near pharynx - Pharyngeal phase cannot occur in synchronized manner (eg. Diphtheria)
- 140. 7/10/2016 Prof.Dr.R.R.Deshpande 140 2) Mastication • Definition - Process of grinding of food under teeth. • Teeth functions - Incisors - To cut the food. • Molars & premolars - Mastication
- 141. 7/10/2016 Prof.Dr.R.R.Deshpande 141 Function of Mastication • Big food particles are converted to small particles. • Surface area increases & digestive enzymes can act better.
- 142. 7/10/2016 Prof.Dr.R.R.Deshpande 142 Muscles of mastication • 1) Temporalis - Originates from temporal bone & is inserted on mandible. Fan shaped muscle. • 2) Masseter - Originates from maxillary part of bone & is inserted on mandible. • Functions - These muscles when contract upward, movement of jaw takes place which helps in grinding
- 143. 7/10/2016 Prof.Dr.R.R.Deshpande 143 Muscles of mastication • 3) Medial & lateral Pterygoid - Located on inner side of mouth. • Due to these muscles side to side movement of jaw occurs which helps in grinding. • All these muscles are supplied by - Mandibular branch of ‘Trigeminal nerve’
- 144. 7/10/2016 Prof.Dr.R.R.Deshpande 144 Mastication Reflex • This is stretch reflex. • Due to presence of food bolus in the mouth jaw drops down. • Stretch receptors in the muscles of mastication are stimulated. • Afferent impulses go through Trigeminal nerve - to its motor nucleus in pons.
- 145. Mastication Reflex • Efferent impulses again via mandibular nerve give signals to the muscle to contract. Jaw is elevated. • Process occurs again & again automatically. • This process can also controlled voluntarily, by motor cortex. We can stop or start the act of mastication voluntarily. 7/10/2016 Prof.Dr.R.R.Deshpande 145
- 146. Mastication – Pathology 1 • Injury or pain or stiffness of TM joint - movement of mastication suffers. • In Tetanus there is a spasm of muscles of mastication - leading to ‘locked jaw’ & mastication reflex suffers. 7/10/2016 Prof.Dr.R.R.Deshpande 146
- 147. Mastication- Pathology 2 • If molars, premolars are in inadequate number - i.e. in the old age → mastication suffers. • If tongue is injured, mastication suffers because for mastication, movements of tongue are helpful to push the food under teeth. 7/10/2016 Prof.Dr.R.R.Deshpande 147
- 148. 3) Movements of stomach • When food enters into stomach it undergoes receptive relaxation. • Then food is stored. • Mixing waves & propulsive waves 7/10/2016 Prof.Dr.R.R.Deshpande 148
- 149. 3) Movements of stomach • Mixing waves are initiated at rate of every 20 sec. & are due BER (Basic Electrical Rhythm). This helps to mixed the food with gastric juice. • Then waves start moving down from fundus to pylorus. They become powerful which increases pressure of antral contents. 7/10/2016 Prof.Dr.R.R.Deshpande 149
- 150. Emptying of stomach • Antral peristalsis (Pyloric pump) & relaxation of pyloric sphincter, releases gastric contents to duodenum. • In stomach food is stored for 2 to 2&1/2 hrs. • It is called as “Gastric emptying time”. 7/10/2016 Prof.Dr.R.R.Deshpande 150
- 151. Emptying of stomach • It can be studied by ‘Barium Meal examination (BA swallow) • Waves of BER, become 5 to 6 times powerful which push fluid food (Chyme) towards pylorus. • This is called ‘Pyloric pump activity’. Emptying of stomach is proportionate to the volume of food 7/10/2016 Prof.Dr.R.R.Deshpande 151
- 152. Factors, which modify, gastric emptying • Stomach factors • Food in the stomach try to hasten gastric emptying. • Stimulation of vagus increases pyloric pump activity & also causes relaxation of sphincter. • Hormone gastrin also has the same effect 7/10/2016 Prof.Dr.R.R.Deshpande 152
- 153. Factors, which modify, gastric emptying • Duodenal factors • With feed back inhibition, distension of duodenum stimulates local nerve plexuses, which inhibit gastric emptying. • Duodenal hormones like GIP & CCK - PZ cause inhibition of gastrin & inhibit gastric emptying 7/10/2016 Prof.Dr.R.R.Deshpande 153
- 154. Factors, which modify, gastric emptying • Fatty food -- Delays gastric emptying. • Chilly food, Protein food has got quick emptying effect. • In pyloric stenosis (which is a complication of chronic duodenal ulcer) Gastric emptying is delayed. 7/10/2016 Prof.Dr.R.R.Deshpande 154
- 155. Enteric nervous system • Nerve supply to Gastrointestinal Tract • There are 2 types of Nerve supply • 1) Intrinsic Nerve supply • 2) Extrinsic Nerve supply 7/10/2016 Prof.Dr.R.R.Deshpande 155
- 156. 1) Intrinsic Nerve supply • Enteric Nerve system is present within the wall of Digestive tract from oesophagus to anus. • Nerve fibers form 2 networks as • i) Auerbach Plexus & ii) Meissner Plexus. These plexuses contain stretch & chemo receptors . • Enteric Nervous system is controlled by Extrinsic nerves. 7/10/2016 Prof.Dr.R.R.Deshpande 156
- 157. 1) Auerbach Plexus • Called as Myenteric Nerve plexus. • It is present in between inner circular muscle layer & outer longitudinal muscle layer. • Main function is to regulate the movements of GI Tract. • Some nerve fibers accelerate the movements by secreting excitatory neurotransmitter like Ach, Serotonin, Substance P. • Other fibers inhibit the GI motility by secreting the inhibitory neurotransmitter like vasoactive Intestinal Polypeptide (VIP), Neurotensin, enkephalin 7/10/2016 Prof.Dr.R.R.Deshpande 157
- 158. 2) Meissner Nerve Plexus • Called as submucous Nerve Plexus • .Present in between the muscular & submucosal layer of GI Tract. • Function is to regulate secretory functions of Digestive Tract. 7/10/2016 Prof.Dr.R.R.Deshpande 158
- 159. 2) Extrinsic Nerve supply • Both Sympathetic & Parasympathetic divisions innervate the GI Tract . 7/10/2016 Prof.Dr.R.R.Deshpande 159
- 160. 1) Sympathetic Nerve Fibers • Preganglionic fibers arise from lateral horns of spinal cord between 5th thoracic & 2nd lumber segments . • They terminate in the celiac & mesenteric ganglia . • Sympathetic nerve fibers inhibit the movements & decrease the secretions of GI Tract. • This happens due to neurotransmitter Noradrenaline .There is also constriction of sphincters 7/10/2016 Prof.Dr.R.R.Deshpande 160
- 161. 2) Parasympathetic Nerve fibers • They pass through some of cranial & sacral nerves . • Nerve fibers to mouth & salivary glands pass through facial & glossopharyngeal nerves. • Preganglionic parasympathetic nerve fibers to oesophagus, stomach, small intestine & upper part of large intestine pass through Vagus nerve. 7/10/2016 Prof.Dr.R.R.Deshpande 161
- 162. 2) Parasympathetic Nerve fibers • Preganglionic fibers to lower part of large intestine arise from 2nd ,3rd ,4th sacral segments & pass through Pelvic nerve. • Parasympathetic nerve fibers accelerate the movements & increase the secretions of GI Tract, with Neurotransmitter Ach. 7/10/2016 Prof.Dr.R.R.Deshpande 162
- 163. 4) Movements of small intestine • Peristalsis - Definition • Wave of relaxation, followed by wave of contraction. • This is the basic property of all tubular structures. • In intestine it is more prominent due to Myenteric plexus 7/10/2016 Prof.Dr.R.R.Deshpande 163
- 164. Types of movement • 1) Mixing movement – • Only 1 segments contracts & relaxes (Segmental peristalsis). • Wave is not spreading to the next segment. • Food is mixed with digestive juices 7/10/2016 Prof.Dr.R.R.Deshpande 164
- 165. Types of movement • 2) Propulsive waves – • Spread from one segment to another & food is pushed ahead & ahead. • Speed = 5 to 6 hrs are required to reach the food from duodenum to Caecum 7/10/2016 Prof.Dr.R.R.Deshpande 165
- 166. Types of movement • 3) Rush peristalsis – • When irritation of mucosa, high segments contracts & large quantity of food is pushed ahead. • Structures lined by smooth muscle 7/10/2016 Prof.Dr.R.R.Deshpande 166
- 167. Types of movement • 4) Anti peristalsis – • Normally wave of peristalsis - From oral to rectal direction. • But when there is excessive irritation (Gastro - enteritis, food poisoning, obstruction) - Waves move in opposite direction, leading to vomiting 7/10/2016 Prof.Dr.R.R.Deshpande 167
- 168. Movements of Villi • Due to movement of submucosa of intestine thin coat of muscle contract due to presence of food & distention of small intestine. • Villi movement help in absorption process 7/10/2016 Prof.Dr.R.R.Deshpande 168
- 169. Role of ilio caecal valve • It allows unidirectional movement of food. • Contents of cecum cannot regurgitate back. 7/10/2016 Prof.Dr.R.R.Deshpande 169
- 170. Causes of Peristalsis • 1) Role of Nerves • i) Role of Myenteric plexus (Intrinsic supply) • In muscularis layer of intestine this plexus is present. Presence of food & distension of intestine stimulate this plexus & they send signal to smooth muscle -increasing movement. • This is called as local reflex/ Myenteric reflex. 7/10/2016 Prof.Dr.R.R.Deshpande 170
- 171. Causes of Peristalsis • ii) Role of sympathetic & parasympathetic nerves (Extrinsic supply) • Parasympathetic nerves - increases the peristalsis. • Sympathetic nerves - decreases peristalsis. 7/10/2016 Prof.Dr.R.R.Deshpande 171
- 172. Causes of Peristalsis • iii) Role of Hormones • CCKPZ, Gastrin, Serotonin etc. hormones directly act on smooth muscle & increase peristalsis 7/10/2016 Prof.Dr.R.R.Deshpande 172
- 173. Functions of Peristalsis • Mixing of food with digestive juices. • Push the food on absorptive surfaces, to facilitate absorption • Undigested food is pushed to large intestine. • To increase the blood supply of intestine. 7/10/2016 Prof.Dr.R.R.Deshpande 173
- 174. Pathology • In cholera, food poisoning - peristalsis is stimulated excessively - which causes loose motion & dehydration. • • Postoperatively or due to anticholinergic drug (Tab Baralgan, Tab Spasmindon) - Movements are reduced. 7/10/2016 Prof.Dr.R.R.Deshpande 174
- 175. Defecation Reflex • Mass peristaltic movement, push faecal matter from sigmoid colon into the rectum. • • Distension of rectal wall stimulates - Stretch receptors. • This receptors send - sensory nerve impulses to the - sacral spinal cord 7/10/2016 Prof.Dr.R.R.Deshpande 175
- 176. Defecation Reflex • Motor impulses, from the spinal cord travel along parasympathetic nerves - back to the descending colon, sigmoid colon, rectum & anus. • Contraction of longitudinal rectal muscle, shortens the rectum, which increases the inside pressure. 7/10/2016 Prof.Dr.R.R.Deshpande 176
- 177. Defecation Reflex • This pressure, along with voluntary contraction of diaphragm & abdominal muscle – -- • Open the internal sphincter & faeces are expelled through the anus. 7/10/2016 Prof.Dr.R.R.Deshpande 177
- 178. Defecation Reflex • If external sphincter voluntarily relaxed - defecation occurs. • But, if it is voluntarily constricted, defecation can be postponed. • In infants, the defecation reflex causes - automatic emptying of the rectum, because voluntary control of the external anus sphincter has not yet developed 7/10/2016 Prof.Dr.R.R.Deshpande 178
- 179. Enzyme - Digestion summary 7/10/2016 Prof.Dr.R.R.Deshpande 179
- 180. Enzyme - Digestion summary 7/10/2016 Prof.Dr.R.R.Deshpande 180
- 181. Faeces • After the last stage of digestion, after absorption of water solid or semisolid waste part is formed which is called as faeces. • Quantity - Roughly about 150 gm of solid stool is passed in 24 hours. 7/10/2016 Prof.Dr.R.R.Deshpande 181
- 182. Composition • If vegetable course cereals & cellulose are excluded from the diet, the faeces show a fairly constant components as follows - • 1) Water - 65 % • 2) Solid - 35 % • i) Ash - 15 % (Mainly, Ca, P4, Fe) • ii) Ether soluble substances (Fat) - 15 % • iii) Nitrogen - 5 % • iv) Other - Desquamated epithelial cells, bacteria, mucous, undigested & unabsorbed food. 7/10/2016 Prof.Dr.R.R.Deshpande 182
- 183. Stool • Reaction - Generally, neutral or acid. • Colour - Due to the presence of Stercobilin, derived from the bile pigments. • Odour - Mainly due to aromatic substances like indole, skatole & also gases like H2S. • Under normal condition about 500 cc of gas is passed out per day. 7/10/2016 Prof.Dr.R.R.Deshpande 183
- 184. Importance of Cellulose • Cellulose serves the important purpose of increasing the bulk of stool & • Thus stimulating the movement of large intestine. 7/10/2016 Prof.Dr.R.R.Deshpande 184
- 185. Faeces formation 1 • Last stage of digestion in the large intestine • The last stage of digestion occurs through bacterial action & no enzymes are secreted by the colon. • Mucus is secreted by the glands of the large intestine, but no enzymes are secreted. • Chyme is prepared for elimination by the action of bacteria. 7/10/2016 Prof.Dr.R.R.Deshpande 185
- 186. Faeces formation 2 • These bacteria ferment any remaining carbohydrates & release hydrogen, CO2 & methane gas. These gases contribute to flatus (Gas) in the colon. • They also convert remaining proteins to amino acids & breakdown the amino acids into simpler substances that is indol, skatole, hydrogen sulphide & fatty acids 7/10/2016 Prof.Dr.R.R.Deshpande 186
- 187. Faeces formation 3 • Some of the Indol & Skatole is carried of in the faeces & contributes to their odour • The rest are absorbed & transported to the liver where they are converted into less toxic compounds & excreted in the urine. • Bacteria also decompose bilirubin into simpler pigments (Stercobilinogen) which gives faeces brown colour. 7/10/2016 Prof.Dr.R.R.Deshpande 187
- 188. Faeces formation 4 • Several vitamins needed for normal metabolism including some B complex vitamins & Vit. K are synthesized by bacterial action & absorbed. 7/10/2016 Prof.Dr.R.R.Deshpande 188
- 189. Absorption & faeces formation • By the time the chyme has remained into large intestine for 3 - 10 Hr. It becomes solid or semisolid as a result of absorption of water & is known as faeces. • Chemically faeces consist of water, inorganic salts, sloughed of epithelial cells from the mucosa of the GI tract, bacteria, products of bacterial decomposition & undigested part of food. 7/10/2016 Prof.Dr.R.R.Deshpande 189
- 190. Physiology of daefecation • 1) Mass peristaltic movements push faecal matter from sigmoid colon into the rectum. • 2) The resulting distension of the rectal wall stimulates pressure - sensitive receptor initiating. Reflex of defecation which results in emptying of the rectum. 7/10/2016 Prof.Dr.R.R.Deshpande 190
- 191. Daefecation • The external sphincter is voluntarily controlled. • If it is voluntarily relaxed defecation occurs, if it is voluntarily constricted defecation can be postponed. • Voluntarily contraction of diaphragm & abdominal muscle aid defecation by increasing the pressure inside the abdomen. 7/10/2016 Prof.Dr.R.R.Deshpande 191
- 192. Daefecation Reflex • In infants the defecation reflex causes automatic emptying of the rectum, without the voluntary control of the external anal sphincter • In certain instances of spinal cord injury, the reflex is abolished & defecation requires supportive measures such as laxative 7/10/2016 Prof.Dr.R.R.Deshpande 192
- 193. Pathology • 1) Diarrhoea - means frequent defecation of liquid faeces, caused by increased motility of the intestine. Since chyme passes too quickly through the small intestine & faeces pass too quickly through the large intestine. There is not enough time for absorption. Vomiting & diarrhoea can result in dehydration & electrolyte imbalance. • 2) Constipation - means infrequent or difficult defecation 7/10/2016 Prof.Dr.R.R.Deshpande 193
- 194. Prof.Dr.R.R.Deshpande • Sharing of Knowledge • FOR • Propagating Ayurved 7/10/2016 194Prof.Dr.R.R.Deshpande